A comparison of canal centering abilities of four root canal instrument systems using X-ray micro-computed tomography
Article information
Abstract
The purpose of this study was to compare the centering abilities of four root canal instrument systems and the amounts of dentin removed after root canal shaping using them.
The mesial canals of twenty extracted mandibular first molars having 10 - 20° curvature were scanned using X-ray micro-computed tomography (XMCT)-scanner before root canals were instrumented. They were divided into four groups (n = 10 per group). In Group 1, root canals were instrumented by the step-back technique with stainless steel K-Flexofile after coronal flaring. The remainders were instrumented by the crown-down technique with Profile (Group 2), ProTaper (Group 3) or K3 system (Group 4). All canals were prepared up to size 25 at the end-point of preparation and scanned again. Scanned images were processed to reconstruct three-dimensional images using three-dimensional image software and the changes of total canal volume were measured. Pre- and post-operative cross-sectional images of 1, 3, 5, and 7 mm from the apical foramen were compared. For each level, centering ratio were calculated using Adobe Photoshop 6.0 and image software program.
ProTaper and K3 systems have a tendency to remove more dentin than the other file systems. In all groups, the lowest value of centering ratio at 3 mm level was observed. And except at 3 mm level, ProTaper system made canals less centered than the other systems (p < 0.05).
I. Introduction
Cleaning and shaping of the root canals is the single most important phase of endodontic treatment1). Canals which seem straight on diagnostic roentgenograms often curve into or out of the flat plane of the film. Teeth with canals that visibly curve mesially or distally often have additional curves not apparent in many planes, and these curvatures should be maintained generally as canal preparation progresses1).
Transportation of the canal in the apical, middle, and coronal thirds has been shown to occur with various instrumentation methods2). However, cleaning and shaping of narrow and curved canals with stainless steel instruments can be difficult and may not provide the optimal shape3).
Shape memory and superelasticity are the main reasons why NiTi alloys have succeeded in endodontics. Files made from Ni-Ti alloy (Nitinol files) in size #15 had two to three times more elastic flexibility in bending and torsion compared with #15 stainless steel files manufactured by the same process, in which the fluted cross-sectional shape was machined directly on the wire blank and suggested that Nitinol endodontic files might be promising for the clinical preparation of curved root canals4). It was reported that there was significantly less transportation of the root canal toward the furcation, and less thinning of the root structure with a Ni-Ti rotary instrument (GT files) compared to stainless steel files in the mid-root sections5). A Ni-Ti rotary instrument (Hero 642) transported canals less, especially at the middle and coronal thirds of the root canals than stainless steel K-files6).
Contemporary available modern NiTi rotary files have unique design properties in terms of cross-sectional geometry. One recent innovation in Ni-Ti rotary instruments is the use of a radial land relief in combination with a positive rake angle in the K3 system. Another active file design was recently introduced as ProTaper, a convex triangular cross-sectional design with an advanced flute design that combines multiple tapers within the shaft.
The purpose of this study was to compare the centering abilities of stainless-steel hand instrument (K-Flexofile) and Ni-Ti rotary instruments (ProFile, ProTaper, K3 systems) and evaluate the amounts of dentin removed after final instrumentation using high-resolution X-ray micro-computed tomography (XMCT) and image software programs.
II. Materials and methods
1. Preparation of specimens
Twenty mandibular molars were selected from fresh extracted teeth without any defect stored in saline solution until used. According to the Schneider's method7), the teeth with 10 - 20° mesial root curvature were chosen. The occlusal surface was ground flat, perpendicular to the long axis of the tooth using diamond disc. The vertical groove was formed on distal root surface near the pulp chamber as a reference point for XMCT analysis.
2. Initial XMCT scanning
Specimens were scanned using XMCT scanner (Skyscan 1072, Skyscan b.v.b.a., Aartselaar, Belgium) at 50 µm interval from the level of working length to the bifurcation area before instrumentation. Approximately 300 cross-sectional images were obtained for each specimen.
3. Root canal preparation
Specimens were randomly divided into four groups (n = 10 canals per group) and prepared using (1) stainless steel K-Flexofile (KF) (Dentsply-Maillefer, Ballaigues, Switzerland) (2) ProFile (PF) system (Dentsply-Maillefer, Ballaigues, Switzerland), (3) ProTaper (PT) system (Dentsply-Maillefer, Ballaigues, Switzerland), and (4) K3 system (SybronEndo, Orange, CA, USA). Size 10 K-Flexofiles were inserted into the mesial canals so that their tips were just visible at the apical foramina, which were separate for both canals. Individual working lengths (WL) were calculated 0.5 mm short of these positions. All canals were prepared up to size 25 at the end-point of preparation. The canals were irrigated between each file with 2.5% sodium hypochlorite. Root canal preparation was done by one operator. All Ni-Ti rotary instruments were rotated at a pre-set r.p.m. and torque following the manufacturer's recommendation using a Tecnika Vision (Dentsply-Maillefer, Ballaigues, Switzerland).
Canal shaping was done as follows:
Group 1 (KF): The coronal part of the canal was flared with Gates-Glidden burs (Dentsply-Maillefer, Ballaigues, Switzerland) from sizes 1 to 3. Each bur was carried passively into the root canal. A size 25 K-file was instrumented to a point of working length. Files were then stepped back in 1mm increments to size 40.
Group 2 (PF): The canals were prepared in a crown-down fashion using ProFile .04 instruments and/or ProFile .06 instruments. A size 25/.04 or .06 ProFile was introduced one half to two thirds of the way down the canal. The instrument was withdrawn when resistance was felt and was followed by a size 30/.04 or .06 ProFile to approximately the same length. A size 20/.04 or.06 ProFile was then used two thirds to three quarters of the way down the canal, and then a size 15/.04 or .06 ProFile was used to the WL. After a size 15/.04 or .06 ProFile reached the WL, a size 20/.04 or .06 ProFile was used to the WL in the same manner. The final apical file size was ProFile 25/.06 instrument.
Group 3 (PT): The canals were enlarged with S1 and S2 used in a gentle pumping and brushing action to the WL. Thereafter, F1 and F2 were used to the WL. The final apical size was F2 file.
Group 4 (K3): First, the canals were prepared in a crown-down fashion using K3 .10 and .08 instruments as orifice openers in the coronal third. Second, K3 40/.06 and 35/.06 instruments were used in the middle third. And last K3 30/.06, 25/.06 and 20/.06 were used in the apical third until true working length was reached. The final apical size was K3 25/.06 instrument.
4. Final XMCT scanning
After root canal preparation, all specimens were scanned using XMCT in the same manner as mentioned above.
5. Measurements and evaluations
All scanned images were processed to reconstruct three-dimensional images using three-dimensional image software (V-works 4.0, Cybermed Inc., Seoul, Korea) and the changes of canal volume were measured. And then, pre- and post-operative cross-sectional images of 1, 3, 5, and 7 mm from the apical foramen were compared (Figure 1). For each level, centering ratio was determined. Centering ratio, reported by Calhoun and Montgomery8), was calculated by the following formula: (T'-T)/D. T'represents the maximum extent of canal movement in one direction and T is the movement in the opposite direction. D is the diameter of the final canal preparation (Figure 2). To obtain these values, pre- and post-operative images were painted with different color and then two images were superimposed after adjusting the opacity of these images using Adobe Photoshop 6.0 (Adobe Systems Incorporated, San Jose, CA, USA). Centering ratio was calculated by image software program (SigmaScan Pro 5.0, Systat Software Inc., Richmond, CA, USA). The data were analyzed by the one-way ANOVA and Scheffe's multiple range tests at 95% significant level using a statistical software SAS (SAS Enterprise Guide 3.0, Cary, NC. USA).
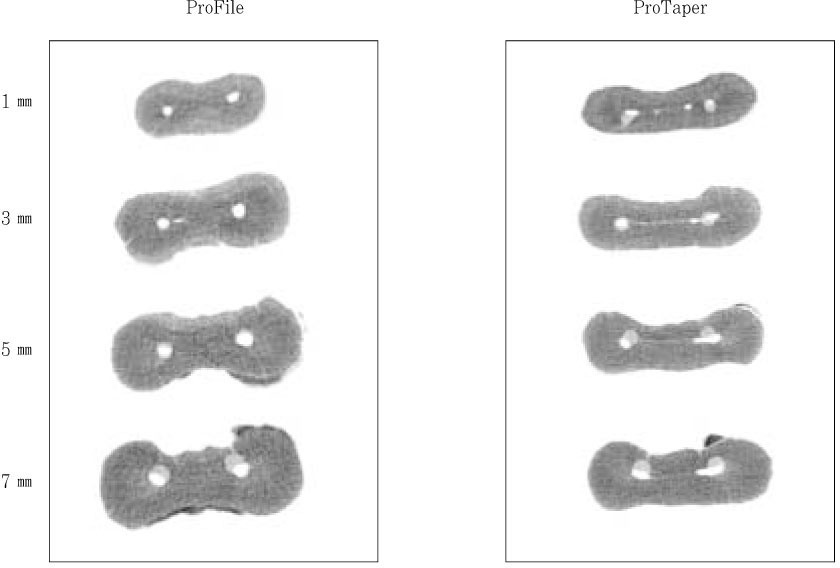
Examples of superimposed images.
Dark gray: Cross section of root after canal shaping
Light gray: Cross section of root before canal shaping

The drawing representing superimposed image of pre-and post-instrumentation canal shapes for measurement of centering ratio.
T': Maximum extent of canal movement in one direction
T: Movement in the opposite direction
D: Diameter of the final canal preparation
III. Results
Change of canal volume
The amount of dentin removed following instrumentation was calculated. Group 3 (PT) and Group 4 (K3) have a tendency to remove more dentin than other file systems. The amount of canal volume change was least in Group 1 (KF), followed in increasing order by Group 2 (PF), Group 3 (PT), and Group 4 (K3). There was no significant difference between Group 3 (PT) and Group 4 (K3) (p > 0.05, Table 1).

Mean change of total canal volume (mm3)

IV. Discussion
A number of techniques are currently available to evaluate the efficacy of instruments to remain centered during root canal preparation. Conventional analytical methods may employ reassembly techniques9), which evaluate cross-sections of root canals before and after preparation. This technique causes some loss of root material because of the thickness and lateral movement of the band saw. Furthermore, some oblique-sectioned surfaces in curved canals could act as ledges that hinder the file from advancing to the working length. Another method, the micro-computed tomography, is emerging in several endodontic research facilities as a nondestructive and accurate method to analyze canal geometry and the relative effects of shaping instruments or techniques10). This innovation was achieved because new hardware and software was available to evaluate the metrical data created by micro-computed tomography, thus allowing geometrical changes in prepared canals to be determined in more detail11). In the present study, using micro-computed tomography, we compared cutting ability and centering ability of various endodontic file systems by calculating the amount of dentin removed and centering ratio, respectively.
The amount of canal volume change was least in Group 1 (KF), followed in increasing order by Group 2 (PF), Group 4 (K3), and Group 3 (PT). Group 3 (PT) and Group 4 (K3) showed almost same results. It assumed that K3 and ProTaper systems have excellent cutting efficiency during instrumentation.
The centering ratio can define the ability of instruments to remain centered in shaped canals. This experiment used a centering ratio formula to evaluate canal transportation. According to this formula, centering ratio approaches zero as T' and T become closer. In the current investigation, all instrumentation systems produced some canal transportation. Especially, ProTaper system made more transportation than other systems except at 3mm level and tended to transport towards the furcation at 5 mm and 7 mm levels.
There are several studies that their findings are consistent with the findings of this experiment. ProTaper removed more canal wall and lessened the canal curvature than did the other instruments12). Bergmans et al.13) reported that the maximum centering ratio was 0.47 for ProTaper system and 0.27 for K3 system, despite of no significant differences between two groups and a center displacement towards the furcation at the coronal section was demonstrated. In this study, centering ratio of K3 and PT system was 0.29 ± 0.04 and 0.45 ± 0.06 at 5 mm level that were similar as the Bergmans et al.'s results. The centering ratio of the Ni-Ti rotary instruments was largest at the 7 mm level and smallest at the 3 mm level in this study, so canal transportation would be larger at the coronal region than at the apical region. The finding of canal transportation was consistent with previous work of Peters et al.14) that canal transportation was prominent at the coronal region in mesiobuccal canals of maxillary molars with significant differences.
Ni-Ti rotary instruments are characterized by different cross-sections and designs of blades. One of the latest trends in NiTi rotary shaft design is the introduction of a radial land relief in combination with a positive rake angle (K3 from SybronEndo). This asymmetrical, more aggressive file design should allow better debris removal, and a cutting rather than a planning action which differs from those possessing U-shaped blades with radial land areas such as ProFile15). It is well known that although there are several factors affecting the cutting efficiency of NiTi rotary systems, the rake angle of the cutting blade plays a central role15). Since dentin is a dense and resilient material, instruments having a negative rake angle are less efficient and require more energy to cut dentin than files with a neutral or positive rake angle16).
A unique feature of the shaping files in ProTaper system is their progressively tapered design, which clinically serves to significantly improve flexibility and cutting efficiency; it typically reduces the number of recapitulations needed to achieve length, especially in tight or more curved canals17). And ProTaper has a convex triangular cross-sectional design. This feature reduces the contact area between the blade of the file and dentin, and serves to enhance the cutting action and improve safety by decreasing the torsional load18). In this study, more aggressive dentin cutting of Protaper resulted in large canal transportation despite of following clinical guidelines suggested by Ruddle18). It may be that as in the present study, the higher values of centering ratio for ProTaper resulted from the absence of radial land area in combination with the large coronal diameter of the ProTaper-shaft13).
In several studies, the shaping ability of different rotary Ni-Ti instruments and stainless steel hand K-files has been compared. In severely curved simulated canals the use of different rotary Ni-Ti instruments such as ProFiles19), GT files20), and K3 instruments21) resulted in less canal transportation compared with stainless steel K-Flexofiles. The present investigation does not corroborate the findings of previous studies. However, Stone et al.22) found that rotary NiTi instrumentation transported the canal more than hand instrumentation. Esposito and Cunningham23) found that NiTi files were more effective than stainless steel files in maintaining the original canal path of curved root canals when the apical preparation was enlarged beyond size 30.
There are many factors affecting the results. Evidence suggests that canal anatomy influences preparation outcomes; significantly more aberrations are recorded when preparing simulated canals with more acute curves in plastic blocks using Ni-Ti rotary instruments24). In addition, three-dimensional analysis using micro CT indicated that canal transportation was more pronounced when shaping narrow curved canals than wider specimens25). Further research is needed to evaluate the characteristics of Ni-Ti rotary systems to determine whether they can be used safely and efficiently in canal shaping procedure.
V. Conclusions
In this study, we compared the centering abilities of four root canal instrument systems and the amounts of dentin removed after final instrumentation using them.
ProTaper system has a tendency to remove more dentin and to transport the original canal towards the furcation more than K-Flexofile, ProFile, K3 system. Further studies will be needed to evaluate the characteristics of each file system in other aspects including three-dimensional analysis of the prepared canal.
Notes
This study was supported by the grant from the Samsung Medical Center (Grant No. C-A5-307-1).