Comparison of shaping ability between various hybrid instrumentation methods with ProTaper
Article information
Abstract
The purpose of this study was to compare and evaluate the shaping abilities of various hybrid instrumentation method using constant tapered file systems with ProTaper® S1 and the difference between experts and inexperienced clinicians in use of NiTi file.
Three hybrid methods used in this study were composed of ProTaper® S1 and K-Flexofile® (group S), ProTaper® S1 and HeroShaper® (group H), and ProTaper® S1 and ProFile® (group P), respectively. The ProTaper®-alone method (group C) was introduced as a control group.
After canal preparation, the lapse of time was recorded. The images of pre- and post-operative canal were scanned and superimposed. Amounts of instrumented canal widths and centering ratio were measured at apical 1, 2 and 3 mm levels and statistical analysis was performed.
In this study, both of the group C and S took more time to prepare canals than other groups. Inexperienced operators required more time for the entire preparation with the groups C and H than the experienced (p < 0.05). And the centering ratio of group P were preferable to ProTaper®-alone method or the hybrid technique using stainless steel files. As such, within experienced operators, group H also showed better results in addition to the group P.
Under these condition, the hybrid methods of each the ProFile® system and HeroShaper® with ProTaper® are recommendable comparative to ProTaper®-alone method. According to the results, the hybrid instrumentation method is a more appropriate method of canal preparation than single file system for narrow or curved canals.
I. Introduction
Root canal instruments manufactured from nickel titanium (NiTi) alloy have been developed in an attempt to overcome the limitations imposed by stainless steel alloys1). NiTi instruments have two to three times higher elastic flexibility and a superior resistance to torsional fracture, compared with similar sized conventional stainless steel instruments1-5).
A number of NiTi rotary systems have been introduced in the market. Most of these systems are typical files generally with a constant tapered shaft design, while they have their own rake angles and radial lands6-10). On the other hand, the recently developed ProTaper system (Dentsply Maillefer, Ballaigues, Switzerland) is unique among these NiTi rotary instruments in that it has a progressively changing tapered shaft design9,10). And the feature of cross-section of ProTaper - convex triangular - is claimed to reduce the contact area between the file and dentin and to make excellent cutting efficiency10). However, the great taper of ProTaper finishing files (F1, F2 and F3) makes a thicker and stiffer instrument especially at the apical portion, when compared to other files with the same apical size. This may attribute not only to the decreased operation time but also to the increased total canal width and deviation value9-11). Several studies showed that ProTaper system produced more aberrations, deformation and straightening of the canal12-14). And then, some researchers suggested that a Ni-Ti file of less taper or U-file design -e.g. ProFile (Dentsply Maillefer, Ballaigues, Switzerland)-should be better for refining of the apical portion of small curved canals because of its greater elasticity15-17).
Judging from these various views, the complex design of ProTaper system capacitates efficient shaping of the coronal aspects of the canal and the relocation of canal orifices, resulting in a straight-line access10,15,16). Therefore, the ProTaper with other file systems can be used in combination to emphasize the advantages of each system. This hybrid concept is to combine instruments of different file systems and use different instrumentation techniques suitable for individual clinical situations, thus the clinicians can achieve the best biomechanical cleaning and shaping results more easily and simply16,17).
The purposes of this study are to compare and evaluate the shaping abilities of various hybrid instrumentation methods, using constant tapered file systems with ProTaper S1, and to compare the differences between experts and inexperienced clinicians in use of NiTi instruments.
II. Materials and Methods
Twenty dentists were divided into two groups depending on the experience in using NiTi file systems - the first group (N) has no practical experience with NiTi file systems but prepared root canal with manual stainless steel files for more than 5 years. The second operator group (E) was composed of endodontists of over 5 years and has experience with rotary NiTi files over 2 years.
The each groups of operators prepared 80 simulated curved root canals in resin blocks (Endo Training Bloc; Dentsply Maillefer, Ballaigues, Switzerland). And each operator of the groups prepared two simulated root canals with four instrumentation methods respectively. The instrumentation methods are as following.
Method C: Control group - ProTaper system (S1, S2, F1 and F2).
Method S: ProTaper S1 and K-Flexofile (Dentsply Maillefer, Ballaigues, Switzerland) apically.
Method H: ProTaper S1 and HeroShaper (Micromega, Besancon, France) apically.
Method P: ProTaper S1 and ProFile apically.
1. Simulated root canals
The simulated root canal blocks used in this study had the working length of approximately 16 mm and about 40° curvature angle. Aqueous methylene blue dye was injected into the canal to enhance the contrast of the pre-instrumentation image. These resin blocks were scanned in a reproducible position with a scanner (Scanjet C8510A, Hewlett-Packard, California, USA), and then the data were stored in a personal computer.
2. Instrumentation
All of the rotary NiTi files used in this study were operated by an electric motor (Tecnika, ATR, Pistola, Italy) set at 300 r.p.m. and torque of 30 (Tecnika motor setting value) in a 16 : 1 reduction handpiece. The stainless steel K-Flexofile was operated by hand with balanced force technique. The instrumented sequence of each experimental group is summarized in Table 1.

The instrumentation procedures
During the procedures, canals were verified the patency with #10 K-file, then irrigated and lubricated with RC-prep (Stone Pharmaceuticals, Philadelphia, USA) repeatedly after instrumentation. All files used in this study were new.
3. Image taking
After the root canal preparation was completed, enlarged canals were filled with Vitapex (Neo Dental Chemical Products co., LTD, Tokyo, Japan). The resin blocks were scanned again in the reproducible position as previously described. The scanned images were assessed on a 15-inch TFT-LCD monitor (SyncMaster CX1565N, Samsung, Suwon, Korea) using Adobe Photoshop ver.7.0 (Adobe, San Jose, California, USA). The pre- and post-instrumented canal images were superimposed on one another and these superimposed images were inspected at a magnification of 141 times.
4. Evaluation
4-1. Aberration
Assessments were made according to the various types of canal aberrations such as apical zip, elbow and ledge.
4-2. Preparation time
Each operator recorded the time lapse of canal preparation including time for irrigation, changing instruments and recapitulation.
4-3. Assessment of canal preparation: Instrumented canal width and centering ratio
Measurements were made horizontally at three levels (1, 2 and 3 mm) from apical foramen (Figure 1). Instrumented canal widths were measured linearly from the pre-instrumented point to the post-instrumented wall inward and outward at each level. The amount of deviation was measured and centering ratio was calculated to evaluate the movement of root canal center after preparation18,19). The ratio was computed using the following method: the absolute value of deviation divided by the whole width of the post-instrumented canal (Figure 2).
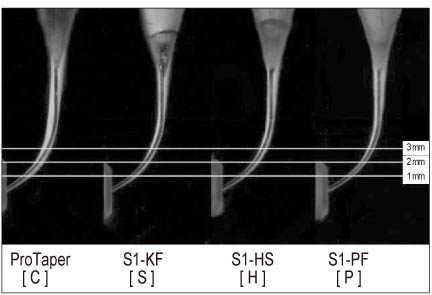
Representative superimposed images after instrumentation by method; the three horizontal lines mean the measured levels of 1 mm, 2 mm and 3 mm from apical end.
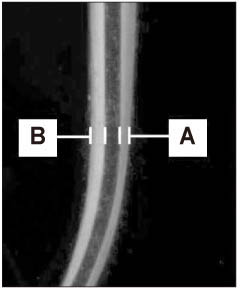
Instrumented canal width and deviation; Deviation: A-B.
A, outward instrumented width
B, inward instrumented width
5. Statistical analysis
Statistical analysis of the collected data was performed with SPSS version 10.0 (SPSS Inc., Chicago, IL, USA). Statistical analysis of the four experimental groups was performed with ANOVA and Duncan's multiple range tests for post-hoc comparison. Independent t-test was done for comparative analysis between operators. Differences revealed in the data were designated as significant at p < 0.05.
III. Results
1. Aberrations
The resin blocks instrumented with group S had more ledges than the other groups (Table 2). The experienced group made no aberrations with any methods.

Incidence of canal aberrations by groups
2. Preparation time
The time needed for completion with each method is presented in Table 3. Both the group C and S took more time to prepare canals than the other groups irrespective of the experience of operators. The inexperienced operators required more time for the entire preparation with the group C and H methods than the experienced (p < 0.05).

The lapse of time (seconds) per group (Mean ± SD)
3. Instrumented canal width and centering ratio
The instrumented canal widths after preparation were diminished in the order of groups C, S, H and P at all levels, regardless of operators (p < 0.05), except at 1 mm in the experienced where showed no significant differences between C and S groups and between S and H groups (Table 4).

Instrumented canal width (µm) after root canal preparation (Mean ± SD)
The centering ratio is a measure of the ability of the instrument to stay centered in the canal18,19). In inexperienced operators, at 1 and 2 mm, group P was distinctive from group H (p < 0.05). Group P had the smallest centering ratio of all the groups (p < 0.05). Group H had significantly larger centering ratios compared with group P (p < 0.05), and had no significant differences with group C (p > 0.05). Comparable with group C, however, group S had a better centering ability at 2 mm, but a larger ratio at 1 mm (p < 0.05) and no significant differences with group C.
Within the experienced operators, there were no significant differences between group P and group H except at 2 mm, and both groups had smaller centering ratios than group C (p < 0.05). Group S had no significant differences with group C at 1 mm levels and the largest ratio than the other hybrid methods (Figure 3 - 4 and Table 5).
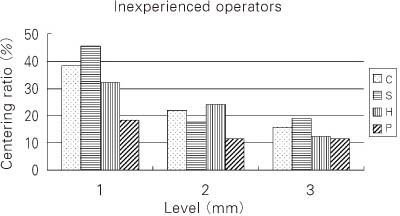
Mean differences of centering ratio between 4 methods in inexperienced operators.
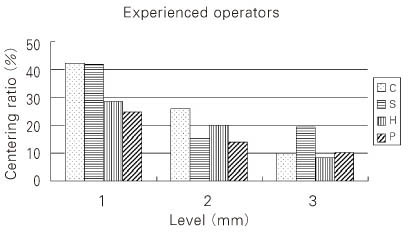
Mean differences of centering ratio between 4 methods in experienced operators.

The significant differences between groups in centering ratio
IV. Discussion
Clinically, it is true that there is no one perfect system of NiTi rotary instruments for all cases of root canal preparation. Each system has its own strong points and shortcomings, and particular rules for its operation. Likewise, ProTaper has many reports regarding its usefulness, especially in the initial phase of shaping (coronal and midroot portion)10,15,16). Despite its several merits, however, some studies showed that the ProTaper instruments produced more aberration, deformation and straightening of the canal especially at the apical portion, due to their thicker and stiffer finishing files (F1, F2 and F3)12,14). Because of these concerns about procedural errors, some studies recommended that the use of passive or manual NiTi files should be better for the final phase of shaping of curved canals as a hybrid technique15,17). It leads to the concept of hybrid instrumentation that can combine the best features of different systems for safe, quick, and predictable results16).
In this study, the hybrid instrumentation methods, combining ProTaper S1 and other instruments, were tested to compare the shaping ability. ProTaper S1 was used for the performance of body shaping and apical pre-enlargement, and the respective subsequent system of K-Flexofile, HeroShaper and ProFile was operated for the shaping and refining of the apical portion.
Conventional stainless steel files have higher deviations and more procedural errors than NiTi rotary files2-6). Up to now, however, stainless steel files are widely used and familiar with dentists using the traditional hand instrumentation techniques, and Szep et al.20) reported that they produced a less occurrence in fracture of files than the NiTi collection. In this study, K-Flexofile was used as the representative of traditional stainless steel files, which is more flexible than the other stainless steel files. HeroShaper and ProFile are active and passive rotary NiTi instruments respectively and generally well acknowledged to the clinician.
One of the main problems inherent in the rotary preparation by clinicians is the risk of instrument fracture21). In this test, however, there was no fracture of instruments but the aberrations that might lead to fracture and hinder ideal canal preparation were distinctively noted in group S (ProTaper S1 and K-Flexofile) by inexperienced operator. Despite the notice, no statistical conclusions could be made by reason of the small number of occurrence.
In order to evaluate canal shaping ability, the time lapse for preparation, instrumented canal width, and centering ratio were measured and calculated18-22,23).
Group C, as the control group, took more time and showed the largest cutting ability and higher apical deviation than other hybrid methods. It is consistent with some other studies in this points11-14). Group S, compared with group C, took less instrumentation time in inexperienced operators and had no differences with experienced operators, in contrast to other reports12-14). It was probably that the operators without experience in rotary files had taken extreme care about active cutting tendency of ProTaper, to follow the recommendation from manufacturer. Another possibility is that they were already familiar to the traditional K-file. Group H and group P took less instrumentation time significantly than the other groups in both operators. Despite the research that the rake angle affects the shaping time24), interestingly, group H did not have significant differences with group P. The result was interpreted that the time lapse was reduced significantly by the use of ProTaper S1 for pre-flaring of coronal two-thirds. Tip diameter of S1 corresponds to ISO size #17, and this made it easy to get not only coronal flaring but also apical preenlargement with the progressive greater taper.
Group S showed that the instrumented widths were smaller than group C at all measured levels. But, both of two groups showed poor centering ability than other two hybrid method. Especially, at 3 mm level, the group S had significantly larger width than other method in both operator groups. It was probable that the elasticity of K-file became problematic as the F series of ProTaper, thereby group S showed some aberrations also, especially in the severely curved canal2-4).
Group P showed the smallest instrumented width at all measured levels. Meanwhile, group P had the tendency of better centering ability than the other groups at all levels.
On the other hand, in group H, the canals were enlarged to larger width than group P, but were less than groups C and S. In addition, it was noticed that group H had similar centering ratios with group P at 3 mm in both operator groups. Particularly, at the 1 mm level (the terminal point of the curvature), group H had larger centering ratio than group P in inexperienced operators, but both groups yielded the similar centering with the experienced operators. The differences observed between groups P and H may be explained by the geometric design of ProFile and HeroShaper and by the difference in experiences of operators. With regards to the instrument design, Powell et al.25) has reported that the tip design of the instrument affects the shape of canals and the levels of deviation.
Canal shaping is disposed to transport the prepared canal away from the original axis. To prevent this problem, Griffiths et al.26) recommended that clinicians need to restrict the use of larger and stiffer instruments in the deeper portion of curved canal. In addition, various preparation techniques have been proposed to minimize this phenomenon. One of the effective methods is to pre-flare the coronal segment, and it is perhaps because of the fact that pre-flaring means that the file tip works on a minor contact surface16,19).
In present study, it was largely attributable to the use of ProTaper S1 that helped prepare a sufficiently wide and smooth-walled glide path in the coronal aspect of the curvature of the canal.
Among these hybrid methods, group P and group H showed good centering, less straightening, transportations and aberrations, in addition to the time-saving properties. These results generally corresponded with the distinguishing characteristics of each file system6-15,27-30). Under this condition, hybrid methods showed better results than ProTaper-alone method, except for group S. Group S, when compared with group C, did not have any advantages in this study. Stainless steel files, however, may be preferable in smaller canals, because these instruments are able to negotiate constrictions and obstructions without bending5). Therefore, clinicians have to make a choice over the instruments and methods suitable for each and individual case.
According to the present results, we can suggest the hybrid instrumentation is a more appropriate method in canal preparation than single file system especially for narrow or curved canals. Under the condition of this study the group P, pre-flaring with ProTaper S1 and apical enlargement with ProFile, can be recommended for overall efficiency. Group H, pre-flaring with ProTaper S1 and apical enlargement with HeroShaper, was preferred for experienced operators in addition to group P, as group H showed more cutting efficacy and centering ratios not significantly different from group P.
For use of this method in clinic, it is necessary to understand where in the canal each instrument performs its cutting action and apprehend when and how to use each instrument to its best ability.
V. Conclusion
According to the present results, we can suggest that hybrid instrumentation is more appropriate canal preparation method than single file systems for narrow or curved canals.
In this study, the centering ratio of group P was preferable to ProTaper-alone method or the hybrid method using stainless steel files. As such, within experienced operators, group H showed better results in addition to the group P. Under these conditions, hybrid methods of the ProFile and HeroShaper system with ProTaper are recommendable comparative to ProTaper-alone method.
Notes
This work was supported by Pusan National University Research Grant, 2004.