Re-establishment of occlusion after unilateral condylar fracture
Article information
Abstract
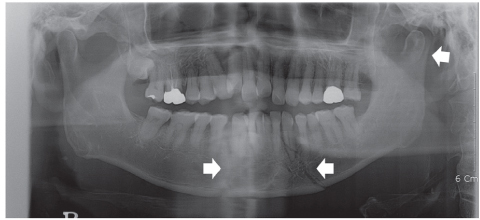
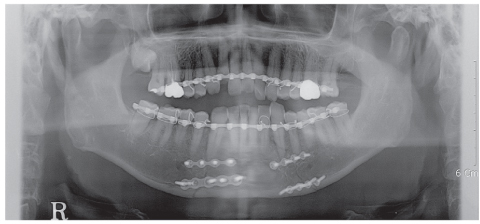
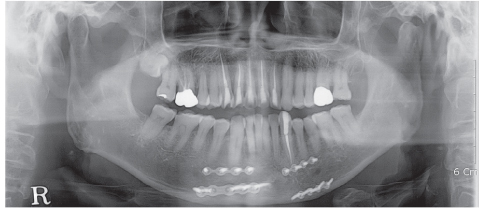
Complications resulting from condylar fracture include occlusal disturbance due to loss of leverage from temporomandibular joint (TMJ). In general, closed reduction with active physical training has been performed, and under favorable circumstances, adaptation occurs in attempt to restore the articulation. The patient in this case report had unilateral condylar fracture accompanied with multiple teeth injuries, but he was left without any dental treatment for 1 mon which led to unrestorable occlusal collapse. Fortunately, delayed surgical repositioning of dislocated maxillary anterior teeth followed by consistent long-term physical training has been proved successful. Normal occlusion and satisfactory remodeling of condyle were obtained on 10 mon follow-up.
Notes
No potential conflict of interest relevant to this article was reported.