A 48-month clinical performance of hybrid ceramic fragment restorations manufactured in CAD/CAM in non-carious cervical lesions: case report
Article information

Abstract
From the restorative perspective, various methods are available to prevent the progression of non-carious cervical lesions. Direct, semi-direct, and indirect composite resin techniques and indirect ceramic restorations are commonly recommended. In this context, semi-direct and indirect restoration approaches are increasingly favored, particularly as digital dentistry becomes more prevalent. To illustrate this, we present a case report demonstrating the efficacy of hybrid ceramic fragments fabricated using computer-aided design (CAD)/computer-aided manufacturing (CAM) technology and cemented with resin cement in treating non-carious cervical lesions over a 48-month follow-up period. A 24-year-old male patient sought treatment for aesthetic concerns and dentin hypersensitivity in the cervical region of the lower premolar teeth. Clinical examination confirmed the presence of two non-carious cervical lesions in the buccal region of teeth #44 and #45. The treatment plan involved indirect restoration using CAD/CAM-fabricated hybrid ceramic fragments as a restorative material. After 48 months, the hybrid ceramic material exhibited excellent adaptation and durability provided by the CAD/CAM system. This case underscores the effectiveness of hybrid ceramic fragments in restoring non-carious cervical lesions, highlighting their long-term stability and clinical success.
INTRODUCTION
Non-carious cervical lesions (NCCLs) are very common in the population, often going unnoticed by the patient and only detected during a dental visit. The prevalence of NCCLs can be around 47%, including their presence in young adults [1]. Diagnosing NCCLs can be challenging due to their multifactorial etiology, but certain aspects might help establish the initial point of the hard tissue loss and other associated factors [2]. Within a multifactorial context, abfraction is one of the factors responsible for the formation of NCCLs. Occlusal stress leads to microfractures of the hydroxyapatite crystals of the enamel and dentin at the cervical portion of the tooth [34]. If the patient applies excessive force while brushing their teeth or uses a highly abrasive toothpaste, there is an increase in the loss of dental tissue due to abrasion [2]. In other cases, the ingestion of erosive liquids can cause softening and dissolution of the most superficial layers, making the substrate prone to suffer more wear and/or microfractures [2].
To treat NCCLs, the etiological factor must be controlled, and the loss of dental structure must be recovered to prevent lesion progression. Direct restorations are a common option for clinicians when addressing these cervical cavities. However, several drawbacks must be overcome, including humidity control, difficult access to the lesions, polymerization shrinkage, polishing procedures that protect the marginal gingiva, and the long clinical time that can cause discomfort for patients [5].
The indirect approach using chairside computer-aided design (CAD) - computer-aided manufacturing (CAM) restorations represents a significant advancement in the treatment of NCCLs [678]. It offers numerous advantages, such as allowing for initial polymerization shrinkage and subsequent post-curing shrinkage to occur before cementation, thereby enhancing the final restoration’s properties compared to the direct technique [9]. Additionally, it facilitates adequate marginal adaptation, precise margin finishing, and polishing, all of which contribute to improved periodontal health [10]. Furthermore, scanning impressions provide greater comfort to patients compared to traditional silicone impressions [11]. On the other hand, implementing the digital protocol necessitates the training and qualification of clinicians, in addition to significant expenses associated with adopting the digital system [12].
Nevertheless, the cost and the time required to fabricate indirect restorations remain an important concern of the technique. Also, like all indirect procedures, it is more complicated compared to direct ones. This requires proper training and experience for practitioners. The use of the chairside semidirect technique overcomes this issue without affecting the restoration quality [9101113]. Recently, a semi-direct technique was suggested as an alternative in anterior and posterior restorations, which has shown good results in the literature, in which the composite resin is applied directly and sculpted on the tooth surface before acid etching and adhesive application [5]. It is then light-activated, removed, and finished extraorally before indirect adhesive cementation, which improves the physical properties and clinical behavior of the finished composite restorations due to increased monomer conversion and facilitates greater operator control over the result. These characteristics are also found in the indirect technique [56].
Considering that this technique might not reduce the number of steps until the final restorative process, the advantages over polymerization shrinkage, polishing extraorally, and appropriate margin adaptation make it worth considering. Despite the elimination of the lab involvement in the restoration fabrication, the procedure allows the realization of a predictable result from both an esthetic and functional point of view, as the restoration is fabricated and corrected chairside [14].
Another important matter for the restoration is the selection of the dental material. Since the cervical portion is prone to stress concentration and biofilm accumulation, the material used should be similar to the tooth structure and achieve a very well-polished surface [315]. Several materials can be used in Class V restorations as direct restorations, such as composite resins, glass ionomers, or a combination of both [161718]. However, each material has some disadvantages. For instance, while glass ionomers show higher retention rates for up to 5 years, composite resins demonstrate better color match and marginal smoothness than glass ionomers [16]. This highlights the necessity of evaluating new indirect materials to improve clinical performance in NCCLs restorations. Hybrid ceramics are a new category of in-office CAD/CAM materials that have been designed to take advantage of the reduced brittleness and increased fracture resistance typical of composite resins combined with the unique aesthetic characteristics of ceramic materials, presenting better mechanical and durability properties than composite resins and glass ionomer [819]. This case report presents the use and performance over 48 months of a hybrid ceramic fragment manufactured in CAD/CAM to restore NCCLs.
CASE REPORT
The case report received approval (6.850.692) from both the Scientific Review Committee and the Committee for the Protection of Human Participants at the local University. The present clinical study was described following the CARE case report guidelines [20]. A 24-year-old male patient complained of aesthetic concerns and dentin hypersensitivity to cold stimuli and during brushing in the lower premolar teeth in the right hemiarch. During clinical inspection, two non-carious cervical lesions were observed on teeth #44 and #45 (Figures 1 and 2), with the presence of an antagonist. The characteristics of the lesions are presented in Table 1.

Intraoral photograph in frontal views of the patient's teeth showing changes in anatomy, color and absence of a carious process in the cervical region, indicating the presence of a non-carious cervical lesion.

Intraoral photograph in lateral views of the patient's teeth showing changes in anatomy, color and absence of a carious process in the cervical region, indicating the presence of a non-carious cervical lesion.

Characteristics of the non-carious cervical lesions
In the clinical evaluation, the patient reported that the lesions had been present for more than 10 years since undergoing orthodontic treatment. This could be a contributing factor to the appearance of these lesions, as no other NCCLs were observed. An occlusal evaluation was conducted to confirm this diagnosis, and it was determined that the patient did not exhibit any occlusal dysfunction. Additionally, the patient maintained good oral hygiene and did not present any carious lesions. Among the different restorative treatments, indirect restorations using hybrid ceramic CAD/CAM blocks were offered to the patient. The patient agreed to this alternative and signed an informed consent form.
Initially, the NCCLs were cleaned with pumice stone and water using a rubber cup. No grinding or cavity preparation was performed. A lip and cheek retractor were positioned for intraoral scanning. One of the operators dried the tooth surface and applied CEREC Powder (titanium dioxide) reflective powder to the teeth. Then, scanning was performed with the CEREC Bluecam camera (Sirona Dental Systems LLC, Charlotte, NC, USA; Figure 3A). Upon acquiring the images, the delimitation of the border lines of the restorations in the CEREC system (Sirona Dental Systems LLC) was conducted, followed by the design of the final restorations. The information was subsequently sent to a milling machine (Sirona Dental Systems LLC; Figure 3B) to produce the final restoration.
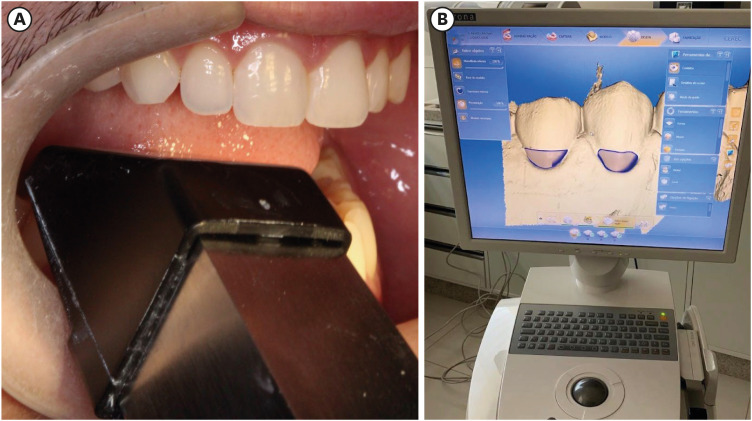
Dental scanning and image acquisition protocol. (A) Dental scanning and (B) image acquisition.
The pieces were made using 14 L hybrid glass-ceramic ceramic blocks (Brava Block; FGM, Joinville, SC, Brazil) (Figure 4) in A2 HT color. The fragments were removed, and hand finishing was carried out.

Pieces of hybrid ceramic blocks (Brava Block; FGM).
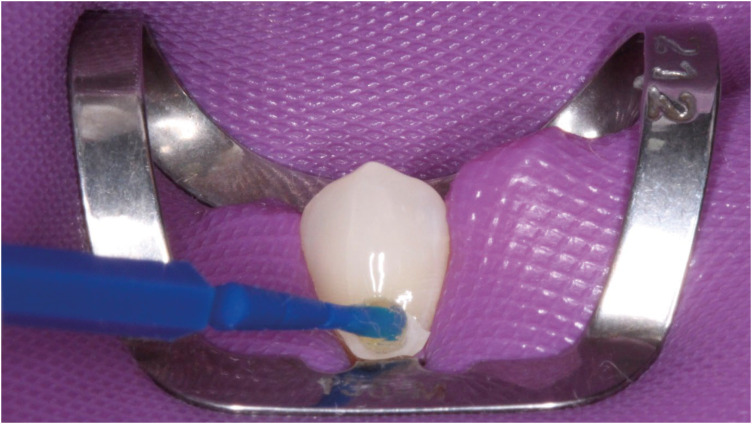
In the same session, the patient was anesthetized with a 3% solution of articaine hydrochloride (Articaine, Nova DFL, Rio de Janeiro, RJ, Brazil) and isolated using a rubber dam (Flexi Dam; Coltene, Altstätten, Switzerland) and 212-retractor clamp. Both NCCLs Both NCCLs were treated in the same session (Figure 5). After the isolation of the NCCLs, it was possible to test the adaptation of the restorations (Figure 6), which was considered satisfactory.

The non-carious cervical lesions after applied the rubber dam.
Test the adaptation of the restorations.
Hybrid ceramic fragment preparation: Sandblasting with 50 µm aluminum oxide at 2 bars (30 psi) for 5 seconds, followed by an ultrasonic cleaning process for 5 minutes, was carried out. Silane (Prosil; FGM) was applied with a microbrush (Cavibrush; FGM) for 1 minute, followed by air drying for 1 minute to remove the remaining solvent (Figure 7A). Afterward, two coats of a universal adhesive (Ambar universal; FGM) were applied with a microbrush (Cavibrush; FGM), with air drying applied for 20 seconds after each coat to evaporate solvent (Figure 7B). To prevent curing from light, the piece was kept away from light.
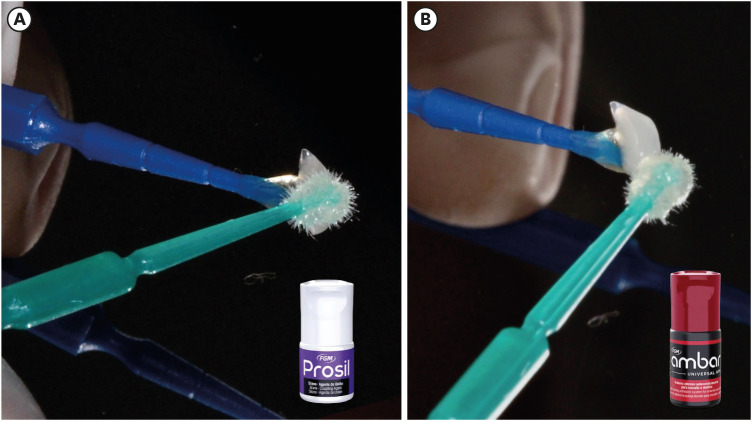
Fragment bonding procedure. (A) Applied silane with a microbrush. (B) Applied Universal adhesive was applied with a microbrush.
Tooth preparation: Selective enamel etching was performed with 37% phosphoric acid (Condac 37; FGM) for 30 seconds (Figure 8A), followed by rinsing with water for 30 seconds. After that, the enamel and dentin were slightly air-dried, keeping the dentin slightly moist (Figure 8B). The universal adhesive (Ambar Universal APS; FGM) was vigorously applied to the dental substrate using a microbrush (Cavibrush; FGM) (Figure 8C). A slight air dry was applied for 20 seconds to remove the solvent. The adhesive was not light-cured due to the potential formation of puddles of the material, which would make it impossible to adapt to the restoration. Immediately afterward, a dual-cure and self-mixed resin cement. For the cementation, the dual cement (Allcem; FGM), was applied with a self-mixing tip directly on the tooth cavity (Figure 8D), followed by the cementation of the restorations (Figure 8E). Before light-curing, excess resin cement was removed with a microbrush (Cavibrush; FGM), and the light-curing procedure was performed for 60 seconds using a 1,200 MW/cm2 unit (Radii; SDI, Bayswater, VIC, Australia) (Figure 8F).
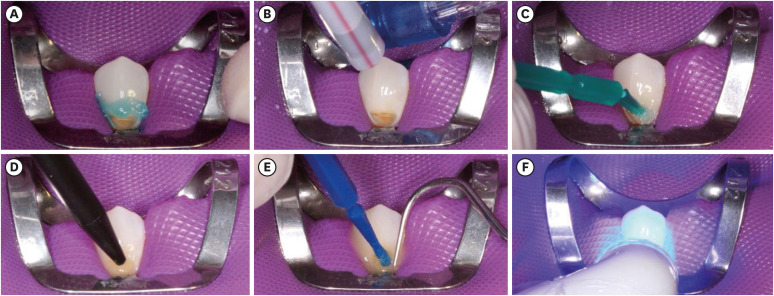
Teeth etching and bonding procedure. (A) Selective enamel etching was performed. (B) Enamel and dentin were slightly air-dried, keeping dentin slightly moist. (C) Applied universal adhesive was applied vigorously on the dental substrate with a microbrush. (D) Applied dual cement on the cavity tooth. (E) Followed by the cementation of the restorations. (F) Light-curing.
The rubber Dam Isolation was removed, finishing was performed with a diamond bur (Figure 9A), and the polishing procedure was conducted with a sequence of discs (Diamond Pro; FGM) (Figure 9B), and a felt disc (Diamond Pro; FGM) (Figure 9C) with diamond paste (Diamond Excel; FGM).
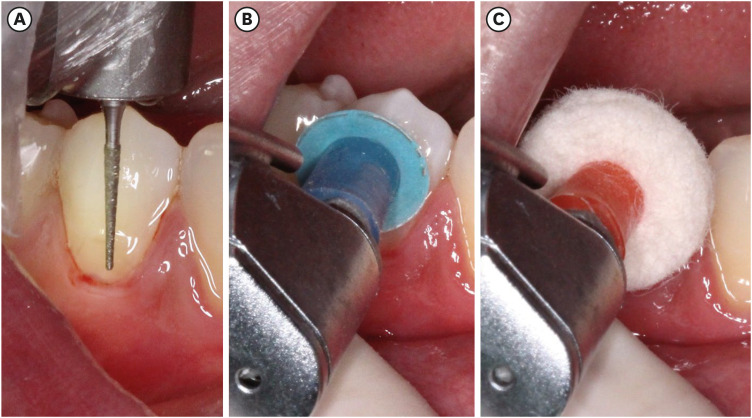
Finishing and polishing procedure. (A) Finishing carried out with a diamond drill. (B) Polishing procedure was performed with a sequence of discs. (C) Polishing procedure was performed with a filter disc.
Restorations immediately after finishing and polishing (Figure 10), after 7 days of treatment (Figure 11), and 48-months after treatment (Figure 12). During the evaluation period, all characteristics described in the revised FDI criteria for evaluating direct and indirect dental restorations, including functional, biological, and aesthetic properties, were assessed and rated as very good or excellent [21]. It is important to note that immediately after treatment, as well as after 7 days and 48 months, the patient expressed high satisfaction with the treatment results. Additionally, the patient did not experience any sensitivity or pain symptoms during these periods.

Restorations immediately after finishing and polishing.

Restorations after 7 days of treatment.

Restorations after 48-month of treatment.
DISCUSSION
Multiple interventions can be performed to restore the aesthetics and structure of NCCLs [22]. With technological processes increasingly present in dental offices, the CAD/CAM system can be an effective tool to treat these situations [7]. With the introduction of hybrid ceramics in the market, it is possible to use them for the manufacture and indication of small fragments for these regions, maintaining the physical and mechanical properties of resin and the brightness and finish of ceramic [23].
The direct approach has been the main method for restoring caries and NCCLs, as the composites can be easily manipulated, inserted, sculpted and activated by light. However, as simple as the direct approach is, there are challenges and difficulties associated with this conventional restorative technique as in the gingival margins for example, and the possibility of future defects. All restorations near the gingival margins of the cavity pose significant challenges. The proximity to the gingival tissue makes it difficult to achieve proper isolation, which is crucial for preventing contamination during the restorative procedure. Contamination can compromise the adhesion of the composite material, leading to poor marginal adaptation and increased susceptibility to marginal staining over time. Additionally, achieving an optimal esthetic outcome can be challenging due to the variations in the gingival contour and color. Over time, these factors can contribute to marginal deterioration, negatively affecting the longevity and esthetics of the restoration. Proper technique and materials are essential to mitigate these issues and ensure a successful outcome [1724].
Currently, hybrid ceramic blocks can be of two types: nanoceramic resin blocks made by high-temperature and high-pressure industrial processes (used in this case report), in which the composite resin (generally containing bisphenol A-glycidyl methacrylate, urethane dimethacrylate, urethane tetramethacrylate, and bisphenol A-diglycidyl methacrylate) is coupled with a ceramic filler (up to 80% by weight) and maintains a high-shine surface finish; and polymer-infiltrated ceramic network (PICN) blocks, formed by a ceramic structure (86% by weight) infiltrated with composite resin (14% by weight), which are indicated for the restoration of a single tooth, such as dental cusp coatings and crowns [25]. Hybrid ceramics have proven to be easier to mill and do not require additional thermal cycles. In addition, they exhibit high flexural strength and can be used even in reduced thicknesses [25].
The restorative material used has great mechanical properties (such as strength, hardness, and wear resistance) [26]. In addition to favorable aesthetics, it has a high gloss, and it is possible to adjust, characterize, and achieve excellent finishing and polishing since it has small particles. In addition, the manufacturing process leads to a higher degree of conversion of CAD-CAM blocks compared to light-cured composites, which could also positively affect the polishing and the final gloss [26].
The bonding procedure of indirect restoration is closely related to the success of the indirect technique. There must be a coupling between the cementing agent and the ceramic material to promote a more effective adhesive interface. However, in zirconia-ceramics, there are lack of silica, making ceramic primers necessary to improve bond strength values to the resin cement and the restorative material. Unlike silica-ceramics or polymer-infiltrated ceramics, hybrid ceramics showed higher bond strength to resin cements compared to resin nanoceramics and zirconia-reinforced lithium silicate materials [27]. The PICN material consists of a dominant ceramic network infiltrated by a lattice polymer [28]. A silane coupling agent proved indispensable for use with silica base ceramic materials because it increases the wettability of the surface and transforms it into a hydrophobic surface, thus increasing the chemical bond and effective interaction with the resin cement [29]. Chemically etching PICN restorations with universal adhesive alone resulted in lower µTBS results than chemical etching with a silane coupling agent. This is likely because the universal adhesive contains insufficient silane to provide chemical adhesion to a silica-based ceramic surface cement [29].
Unfortunately, clinical trials, especially in NCCLs, with these materials are limited. A few 3-year clinical papers report a survival rate of 97.4% for inlays and 95.6% for overlays [30]. Fathy et al. [8], in their systematic review, indicate that CAD/CAM resin-matrix ceramics used for inlays, onlays, or overlays have a success rate of 85.7% to 100.0% across the 7 studies reviewed. However, they caution about the lack of longitudinal studies to provide evidence of satisfactory clinical results. Additionally, the composition of the blocks can vary between brands, and the results are material-dependent, making comparisons between studies very difficult [31].
Hybrid ceramics have promising results in the literature, and their flexural modulus advantages make the material a good choice for cervical regions where flexural stress is concentrated [32]. The greatest benefits of this technique are precise extra-oral margin finishing and polishing and overcoming challenges associated with field control, composite handling, maintaining periodontal health, and polymerization shrinkage stress tensions. A randomized clinical trial that evaluates the retention of these materials in NCCLs is necessary to confirm the effectiveness of the material.
CONCLUSIONS
The CAD/CAM hybrid ceramic fragments have proven to be a valid material for the restoration of NCCLs, providing excellent clinical performance after 48 months.
ACKNOWLEDGEMENTS
The authors express gratitude to FGM (Joinville, SC, Brazil) for the generous donation of the products used in this study. Special thanks to the Bleaching & Bond group (Instagram@bleachingbond; Brazil) for their invaluable assistance throughout all stages of the clinical trial. This study received partial support from the National Council for Scientific and Technological Development (CNPq) under grants 304817/2021-0 and 308286/2019-7, as well as the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior, Brasil (CAPES), Finance Code 001.
Notes
Funding: This study was partially supported by the National Council for Scientific and Technological Development (CNPq) under grants 304817/2021-0 and 308286/2019-7 and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES) – Finance Code 001.
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: Favoreto MW, Martini EC, Matos TP, Bandeca MC, Loguercio AD.
Data curation: Favoreto MW, Cochinski GD, Martini EC, Matos TP.
Funding acquisition: Bandeca MC, Loguercio AD.
Investigation: Favoreto MW, Cochinski GD, Martini EC, Matos TP, Bandeca MC, Loguercio AD.
Methodology: Favoreto MW, Loguercio AD.
Project administration: Loguercio AD.
Resources: Favoreto MW, Cochinski GD, Martini EC, Matos TP, Bandeca MC, Loguercio AD.
Supervision: Bandeca MC, Loguercio AD.
Validation: Favoreto MW, Cochinski GD, Martini EC, Matos TP, Bandeca MC, Loguercio AD.
Visualization: Favoreto MW, Cochinski GD, Martini EC, Matos TP, Bandeca MC, Loguercio AD.
Writing - original draft: Favoreto MW, Cochinski GD, Martini EC, Matos TP, Bandeca MC.
Writing - review & editing: Loguercio AD.
