Procedural errors detected by cone beam tomography in cases with indication for retreatment: in vivo cross-sectional study
Article information

Abstract
Objectives
This study aimed to investigate the frequency and type of endodontic procedural errors in cases indicated for retreatment through cone-beam computed tomography (CBCT) analysis.
Materials and Methods
The sample consisted of 96 CBCT scans, encompassing 122 permanent teeth with fully formed roots. Errors included perforation, instrument fracture, canal transportation, missed canals, and inadequate apical limit of filling. Additionally, potential risk factors were analyzed and subjected to statistical modeling.
Results
The most frequent procedural error observed was the inadequate apical limit of filling, followed by canal transportation, perforation, missed canal, and instrument fracture. Statistically significant associations were identified between various procedural errors and specific factors. These include canal transportation and root canal wall, with the buccal wall being the most commonly affected; missed canal and tooth type, particularly the palatine and second mesiobuccal canal canals; inadequate apical limit of filling and root curvature, showing a higher deviation to the mesial direction in severely curved canals; inadequate apical limit of filling and the presence of calcifications, with underfilling being the most frequent; canal transportation and periapical lesion, notably with deviation to the buccal direction; and the direction of perforation and periapical lesion, most frequently occurring to buccal direction.
Conclusions
CBCT emerges as a valuable tool in identifying procedural errors and associated factors, crucial for their prevention and management.
INTRODUCTION
The primary goal of endodontic treatment is to reduce microbial load, aiming to eliminate the intracanal infection to levels compatible with the healing of the periapical tissues [1]. Nonetheless, 5%–20% of endodontic treatments result in post-treatment apical periodontitis, often attributed to anatomical variations that pose challenges and contribute to procedural errors [2]. These errors include perforations, instrument fractures, canal transportation, missed canals, and inadequate filling [34]. Factors such as root canal calcifications and pulp stones, occurring in 5.1% and 8% of cases, are commonly associated with procedural errors in endodontic practice [5].
The most common treatment alternative for cases with persistent periapical lesions is endodontic retreatment, particularly recommended for inadequately treated cases [6]. However, retreatments are challenging in cases presenting procedural errors. Therefore, meticulous treatment planning, with attention to detail, is crucial to the successful resolution of these cases. In this regard, cone-beam computed tomography (CBCT) stands out as a valuable tool for identifying endodontic procedural errors. The 3-dimensional (3D) nature and high-quality imaging of CBCT offer optimal conditions for error analysis. Despite the availability of this advanced imaging technology, it is noteworthy that several CBCT studies have predominantly examined individual procedural errors, thereby limiting a comprehensive understanding of the various factors influencing treatment outcomes [78].
The present study aimed to investigate the frequency and type of endodontic procedural errors in cases indicated for retreatment through CBCT analysis. Additionally, potential risk factors were analyzed and subjected to statistical modeling.
MATERIALS AND METHODS
This cross-sectional descriptive study received approval from the Institutional Research Ethics Committee (approval No. 209552).
Sample selection and evaluation
A sample calculation estimated the number of CBCT scans required to test pairwise associations between variables. This calculation took into account findings from similar prior studies [910]. Given the variability in these findings, 3 sample calculations were performed, each based on different assumptions: a weak association (r = 0.3), a moderate association (r = 0.55), and a strong association (r = 0.8). With a 5% alpha error and a 20% beta error, the minimum number of scans needed was estimated to be 85.
The sample consisted of 96 CBCT scans, encompassing 122 permanent teeth with fully formed roots and radiographic evidence of previous endodontic treatment, with retreatment indication. CBCT’s indications were based on the 7th and 8th recommendations of the AAE/AAOMR position statement [11]. The data collection occurred between January 1st, 2020 and June 30th, 2022. The scans were obtained using the GIANO HR CBCT equipment (NewTon, Imola, Italy), with FOV limited to 6 × 6 mm, a voxel from 68 to 300 μm, 16 mAs, 90 kVp, and a scan time in the Best Quality function of 16.8–3.6 seconds.
Two examiners underwent training and calibration under the guidance of an expert radiologist with over 10 years of experience in CBCT image measurement, interpretation, and diagnosis. This training was performed with a set of 20 CBCT scans and was focused on standardizing CBCT evaluation. CBCT evaluation was performed using Horos software version V3.3.6 (HOROS, Horos project, Annapolis, MD, USA). Scans were excluded if visualization difficulties due to artifacts were noted by at least 1 examiner. From an initial sample of 120 scans, 24 were excluded due to artifacts, resulting in the 96 that composed the final sample. Substantial agreement between observers was achieved (Kappa value of 0.90). In cases where there was no consensus in the evaluation, a joint review was conducted until consensus was reached.
Evaluation of procedural errors
1. Perforation and direction
The prevalence and direction of perforations were analyzed across the 3 tomographic sections, with greater emphasis on the axial and sagittal sections. The aim was to identify whether perforation occurred and its location within the root canal—whether buccal, distal, mesial, or palatal (Figure 1).
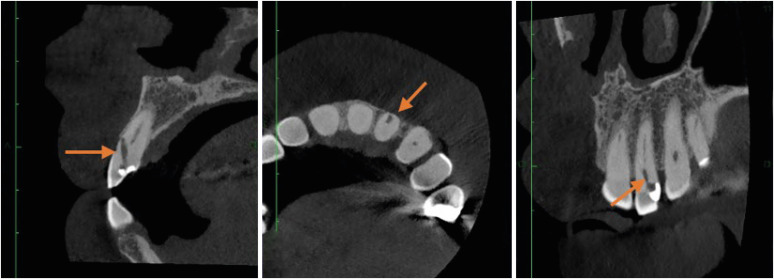
Dynamic cone-beam computed tomography analysis for identification of perforation in the right lateral incisor.
2. Instrument fracture
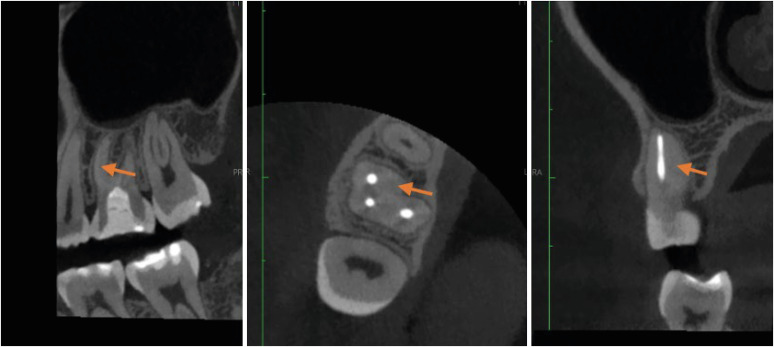
The frequency of instrument fracture was assessed, and the location of the instrument fragment within the root canal was identified (apical, middle, or coronal third). Special attention was given to analyzing sagittal and axial slices of the CBCT (Figure 2).
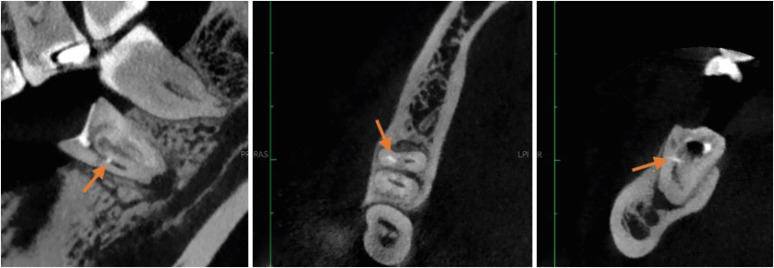
Dynamic cone-beam computed tomography analysis for identification of fractured instrument in lower left first molar.
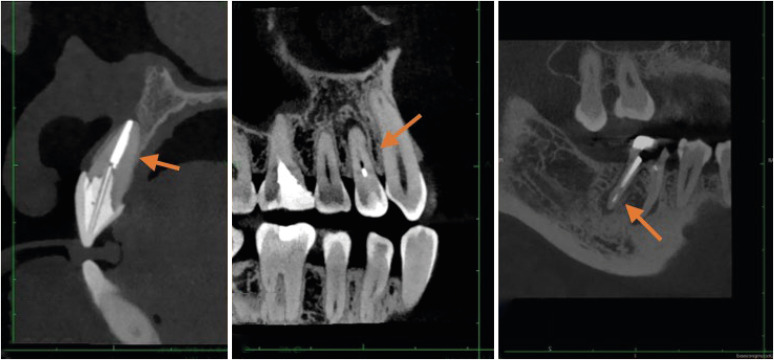
3. Canal transportation
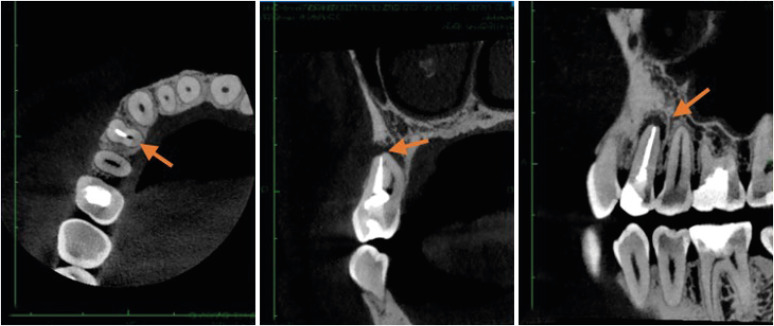
The filling material trajectory was compared with the canal direction, and any detected deviations were categorized as buccal, distal, mesial, or palatal. Evaluation involved analysis of sagittal, axial, and coronal sections of the CBCT (Figure 3).
Dynamic cone-beam computed tomography analysis for identification of canal transportation in upper right first molar.
4. Missed canal
Teeth images were analyzed for the occurrence of at least 1 untreated canal, defined as those without any evidence of filling material from the coronal orifice to the apex, and its association with the presence of apical periodontitis, primarily assessed on axial section images (Figure 4) [12].
Dynamic analysis of cone-beam computed tomography for identification of missed canal.
5. Apical limit of filling
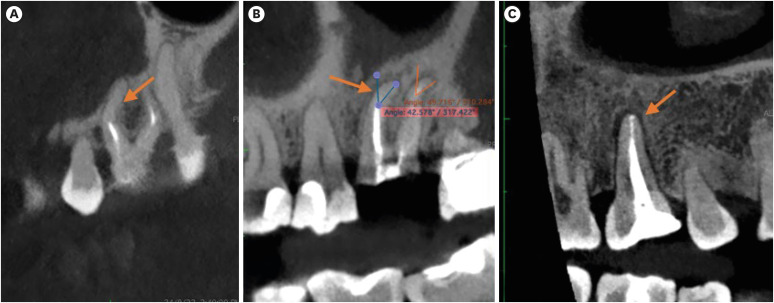
The extent of filling was evaluated using a nominal scale: underfilled (> 2 mm short from the apex), overfilled, both understandable as inadequate, and adequate (0–2 mm short from the apex). Initial assessment was conducted on sagittal section images, with confirmation on axial slices (Figure 5).
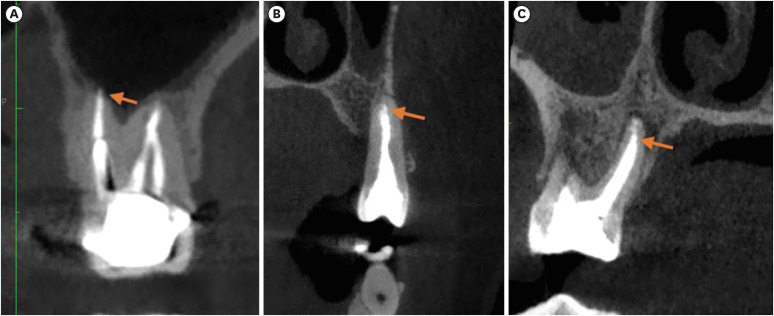
Identification of (A) molar with an overfilled canal, (B) premolar at the appropriate level and (C) palatal canal of an underfilled upper molar.
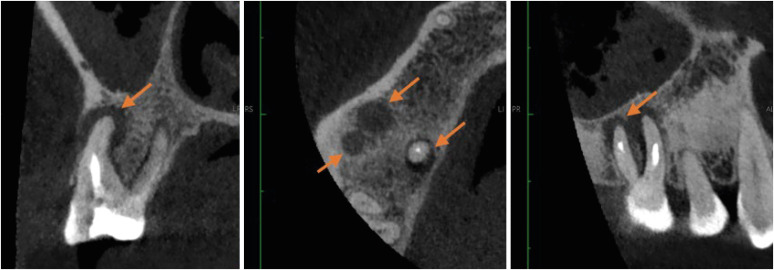
6. Associated factors
Several associated factors were also evaluated: (a) presence of calcifications (Figure 6); (b) tooth type (anterior, premolars, and molars) (Figure 7); (c) periapical lesion, defined by disruption of lamina dura continuity and the presence of a radiolucent area around the root apex at least twice as thick as the normal periodontal ligament space (Figure 8); and (d) root curvature angle according to the Schneider’s method, modified by the inclusion of one more category (mild curvature) (Figure 9) [1314].
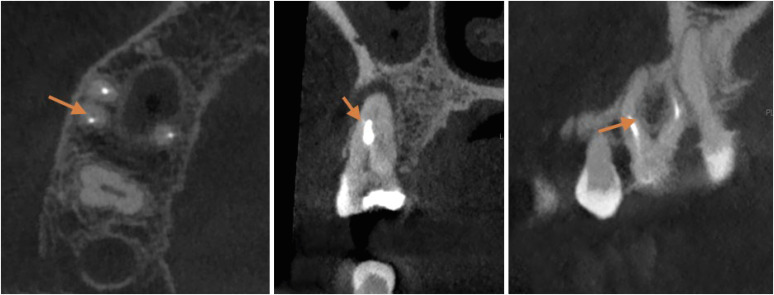
Identification of second mesiobuccal canal calcification in upper left first molar.
Identification of anterior, premolar and molar tooth type.
Identification of periapical lesion in upper right first molar.
Identification of type of curvature, (A) moderate, (B) severe and (C) straight.
Statistical analysis
The data were analyzed using Stata software v. 17 (StataCorp, College Station, TX, USA). Descriptive statistics were computed to understand the distribution of variables via univariate analysis. Absolute and relative frequencies were obtained and represented with tables. For inferential statistics, bivariate analysis was conducted between dichotomous qualitative variables utilizing χ2 and Fisher's analysis. These tests determined the association between endodontic procedural errors and associated factors. Response categories with counts less than 5 were collapsed to ensure statistical robustness.
RESULTS
The most frequent procedural error observed was the inadequate apical limit of filling (82.38%, n = 187), followed by canal transportation (68.72%, n = 156), canal perforation (63.44%, n = 144), missed canal (16.30%, n = 37), and instrument fracture (1.76%, n = 4). For a detailed prevalence of each procedural error, please refer to Table 1.

Type and frequency of endodontic procedural errors per canal (n = 227)
Statistically significant associations (p < 0.01) were identified between various procedural errors and specific factors. These include canal transportation and root canal wall, with the buccal wall being the most commonly affected; missed canal and tooth type, particularly the palatine and second mesiobuccal canal (MB2) canals; inadequate apical limit of filling and root curvature, showing a higher deviation to the mesial direction in severely curved canals; inadequate apical limit of filling and the presence of calcifications, with underfilling being the most frequent; canal transportation and periapical lesion, notably with deviation to the buccal direction in these cases; and the direction of perforation and periapical lesion, most frequently occurring to buccal direction. Conversely, no statistically significant association was found between endodontic procedure error and tooth quadrant (p > 0.05). Detailed frequencies are provided in the respective Tables 2, 3, 4, 5, 6.

Procedural errors according to tooth type

Procedural errors according to the type of root curvature

Procedural errors according to the presence of calcifications

Endodontic procedure errors according to the presence of periapical reaction

Procedural errors according to dental quadrant
DISCUSSION
In contemporary endodontics, the importance of CBCT to assess the quality of previous endodontic treatment is well recognized being probably the greater ally of the clinician to obtain accurate diagnosis and decision-making, especially in cases of posttreatment apical periodontitis [1213]. Using CBCT, the present study significantly advances the understanding of conditions associated with failures in endodontic procedures. By incorporating factors such as root canal anatomy, tooth type, presence of periapical lesion, and root curvature angle, this research highlights aspects often overlooked in similar studies, offering a detailed perspective on how these factors collectively impact endodontic outcomes [78]. This approach contributes to a more comprehensive understanding of endodontic procedural failures.
In this investigation, underfilling emerged as the most prevalent endodontic procedural error, affecting 50.22% of the cases. This finding aligns with previous research, including a study by Nascimento et al. [15] which identified insufficient filling of root canals as the predominant procedural error (52.47%). Similarly, a previous study found underfilled canals to be the most prevalent error (85.9%), with a statistically significant association noted in teeth exhibiting straight curvature (22.6%)—specifically, Vertucci type I—and the presence of a periapical lesion (77.3%) [16]. Moreover, a cohort study evaluating 1259 endodontically treated teeth observed that insufficient obturation, extending beyond or shorter than 2 mm from the apex, significantly reduced the odds ratio for treatment success [17].
Regarding associated factors, a higher prevalence of underfilled canals was observed in straight roots (29.52%), consistent with findings from a previous study, where underfilled canals were significantly more prevalent in teeth with straight canals (22.6%) [16]. Another factor associated with underfilled canals was the presence of periapical lesions, aligning with a previous study [18]. Inadequate filling allows bacteria and other microorganisms to invade the root canal or provide space for those that persist after treatment to proliferate, thereby maintaining or contributing to the development of post-treatment apical periodontitis [19]. The high prevalence of inadequate apical filling limits underscores several critical challenges in endodontic procedures. Technical difficulties in achieving an optimal apical seal. This issue is compounded by the clinician's skill and experience, as less experienced operators may struggle to prepare and thoroughly clean the apical region, jeopardizing the filling procedures.
Canal transportation, the second most prevalent error in our study (28.19%), demonstrated significant associations with the buccal wall of upper incisors, consistent with previous research [20]. The fact that the access cavities of upper incisors are angulated in the palatal direction, makes the buccal canal wall more susceptible to deviations and perforations. Studies have indicated that an apical transposition of more than 0.3 mm compromises the success of canal treatment and increases the risk of canal perforation [2122]. This should be considered a limitation of the present study since the degree of transportation was not evaluated, but only its presence or absence.
The prevalence of perforations was 23.79%, with significant associations observed between perforation direction towards the buccal wall and the presence of periapical lesions. Perforations become a contributing factor to the persistence or recurrence of infection. In addition, it may expose the tooth root to the oral cavity [23]. However, the present results should be analyzed carefully concerning the association of procedural errors with tooth type. For instance, incisors and canines are more susceptible to having more perforations to the buccal side, given the nature of the access cavity. Similarly, canal transportation tends to occur on the outside of the curvature. Therefore, some results depend on the nature of the tooth being analyzed.
Missed canals accounted for 16.29% of the cases, consistent with previous studies reporting percentages ranging from 12% to 23% [1213]. The most frequent missed canals were the palatal and MB2 from the upper molars, aligning with existing literature demonstrating a high prevalence of missed MB2 canals in the upper first and second molars [1213].
Our study revealed a statistically significant association between missed MB2 canals and severely curved upper molar roots, consistent with previous research, which emphasized the importance of 3D examinations in identifying curved canals that may be missed otherwise [24]. Conversely, missed palatal canals in upper premolars were associated with straight canals, in line with previous findings indicating a similar association in maxillary second premolars [25]. Besides, associations between missed palatal canals and the presence of calcifications were evident in the present study, highlighting the impact of calcifications on procedural errors. Notably, CBCT is an indispensable diagnostic tool for surgical and non-surgical retreatment cases, although its superiority varies depending on the specific condition being diagnosed.
Instrument fracture, despite being the least frequent error (1.76%) in the present study, poses challenges in diagnosis via CBCT, with periapical radiographs remaining the preferred diagnostic modality [26]. However, there is a growing trend among clinicians to rely on CBCT for making decisions regarding the management of fractured instruments [27].
CONCLUSIONS
In conclusion, underfilled canal was the most frequent error, especially in straight canals, irrespective of calcifications. Notably, canal transportation in upper incisors correlated with the buccal wall and the presence of periapical lesions. Missed canals were predominantly associated with severely curved mesiopalatal canals, palatal canals, and the presence of calcifications. Perforations were also frequent, particularly in cases with periapical lesions. CBCT emerges as a valuable tool in identifying procedural errors and associated factors, crucial for their prevention and management.
Notes
Funding: This study was supported by grants from Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ) and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Brazilian Governmental Institutions.
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: Valverde Haro HP, Rupaya CR.
Data curation: Valverde Haro HP.
Formal analysis: Valverde Haro HP.
Funding acquisition: Valverde Haro HP.
Investigation: Valverde Haro HP.
Methodology: Rupaya CR.
Project administration: Rupaya CR.
Resources: Valverde Haro HP.
Software: Valverde Haro HP.
Supervision: Rupaya CR.
Validation: Alves FRF.
Visualization: Valverde Haro HP.
Writing - original draft: Valverde Haro HP, Alves FRF.
Writing - review & editing: Alves FRF.





