Single-session associative protocol for dentin hypersensitivity management: a 1-year randomized, blinded clinical study
Article information

Abstract
Objectives
This study aimed to establish a single-session associative protocol for non-restorative management of dentin hypersensitivity (DH).
Materials and Methods
Twenty-four individuals with DH and a minimum sensitivity level of 4 on the visual analog scale (VAS) were selected. The study was conducted in a split-mouth design, with each participant (n = 20) having at least 1 affected tooth in all quadrants. The management protocols consisted of control group: universal adhesive, Neural Desensitizing Protocol group: 5% potassium nitrate, Mixed Desensitizing Protocol (PAM) group: 5% sodium fluoride and 5% potassium nitrate, Remineralizing Desensitizing Protocol (PDR) group: surface-partially reacted glass technology photopolymerizable varnish. Evaluations were performed immediately after application, at 1 week, 1 month, 2 months, and 12 months using the VAS sensitivity test.
Results
The scores were subjected to statistical analysis using the Friedman test (p < 0.05), Durbin-Conover test (p < 0.05), and Wilcoxon test (p < 0.05). At the 12-month evaluation, all groups showed statistically significant differences compared to the initial assessment. For the evaluation after 12 months, there was a statistically significant difference between the PAM group, the control group, and the PDR group.
Conclusions
It can be concluded that all groups were effective in controlling DH, but there were significant results in the control group and PDR group. The clinical relevance of this study is to demonstrate that the application of single-session desensitizing protocols can be effective in controlling DH for up to 12 months.
Trial Registration
Brazilian Clinical Trials Registry Identifier: RBR-4r63d7s
INTRODUCTION
Dentin hypersensitivity (DH) is a prevalent clinical manifestation characterized by acute and short-lasting pain without association with any pathology [123]. Its etiology can be associated with dentin exposure, resulting from the loss of dental enamel or exposure of root surfaces [45]. This loss can occur after periodontal therapy, parafunctional habits, acidic diets, or inadequate brushing [6].
DH is commonly associated with non-carious cervical lesions, which are the manifestation of dental structure loss in the cementoenamel junction (CEJ) and not related to dental caries [7]. The loss of dental structure in the CEJ leads to a response to external stimuli (tactile, thermal, chemical, or osmotic), causing discomfort and reducing the quality of life [8]. The most accepted theory for describing DH is the hydrodynamic theory proposed by Braennstroem and Astroem [8], in which intratubular fluid movement occurs when dentin is exposed to stimuli, resulting in acute and short-lasting pain.
The diagnosis can be made through clinical tests such as the evaporative test, tactile test, or by excluding other painful pathologies [91011]. The main methods of control involve the use of neural agents, obliterating agents, mixed approaches, and associated protocols. Neural agents act on the transmission of nerve impulses by depolarizing the extracellular concentration of ions in neural membranes, preventing repolarization, and consequently reducing the symptoms of DH [12]. Obliterating agents work by sealing dentinal tubules through protein precipitation, remineralizing the structure, sealing the tubules, and reducing fluid flow within the tubules [13].
Recently, a photopolymerizable varnish with bioactive properties has been introduced in the dental market. This varnish releases ions that assist in the control of DH through the process of remineralization, in addition to providing a hermetic seal on the dental surface [14]. This material contains surface-partially reacted glass particles, composed of a bioactive trilaminar structure, and ions such as sodium, aluminum, borate, silicate, fluoride, and strontium, each with specific actions that work synergistically to control DH and prevent dental caries by remineralizing the dental surface [151617].
Fluoride, borate, aluminum, and silicate have antibacterial properties, while strontium, sodium, and aluminum neutralize acids produced by bacteria, reducing the formation of dental biofilm [17181920]. Fluoride transforms hydroxyapatite into fluorapatite, and strontium binds to hydroxyapatite, forming strontium-apatite, providing dentin protection and greater resistance to temperature and pH changes [2122].
The application of an associative protocol involving the use of neural agents followed by obliterating agents in a single clinical session may represent a promising alternative to maximize their benefits [23]. This sequence cannot be altered due to the mechanism of action of the agents used, where the neural agent is applied first to depolarize the nerve fibers, followed by the obliterating agent to seal the dentinal tubule openings. The hypothesis of this study is that the application of an associative protocol using neural agents followed by obliterating agents in a single clinical session will result in a significant reduction in DH due to the synergistic combination of the depolarizing and sealing effects on dentinal tubules provided by the agents used.
MATERIALS AND METHODS
Ethics approval and protocol registration
The experimental design followed the Consolidated Standards of Reporting Trials (CONSORT) statement (Sarkis) and was registered in the Brazilian Clinical Trials Registry (RBR-4r63d7s). The study protocol was reviewed and accepted by the Local Ethics Committee on Investigations Involving Human Subjects (CAAE 25889819.6.0000.0107). All patients who met the selection criteria were informed of the study's objectives, procedures, risks, and benefits and expressed consent to participate by signing the Terms of Free and Enlightened Consent.
Trial design, settings, and recruitment
This randomized, prospective, double-blind, and parallel clinical trial was conducted between September 2021 to October 2022. This randomized clinical trial had dentin sensitivity as the outcome evaluated, and the variation factor was follow-up times. The participants were recruited through advertisements published in the local community.
Randomization, allocation concealment, and blinding
This controlled clinical trial had an equal allocation rate to the groups. Based on the inclusion and exclusion criteria, the selected teeth were divided into 4 groups using block randomization (4 × 5) of the Research Randomizer software version 4.0. During the application of the interventions experiments, the patient did not know to which experimental group belonged, not allowing this to interfere with the patient's perception of sensitivity. According to the CONSORT flow diagram, the distribution and dynamics of the groups are shown in Figure 1.
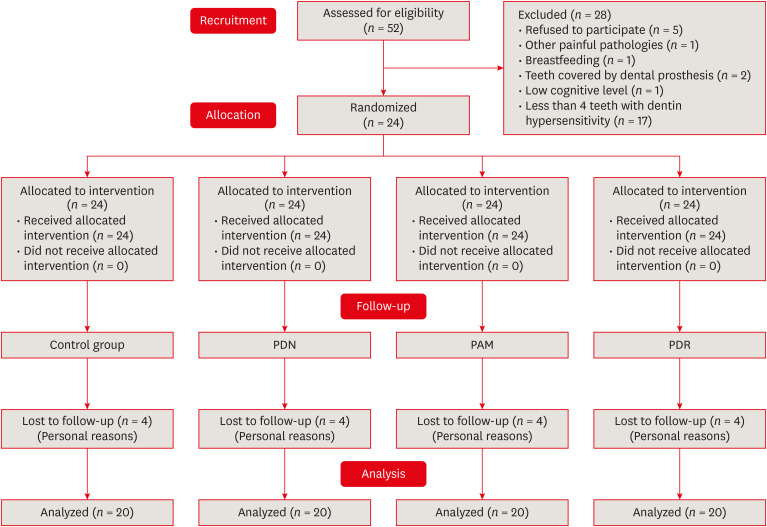
Search method flowchart.
PDN, Neural Desensitizing Protocol; PAM, Mixed Desensitizing Protocol; PDR, Remineralizing Desensitizing Protocol.
Eligibility criteria
Individuals aged 18 to 60 years, both sexes, without systemic compromise, non-smokers, with at least 4 teeth with DH (at least 1 tooth per quadrant) on the buccal surface, sensitive to evaporative stimuli, with gingival recession equal to or less than 2 mm, without using methods to control DH in the last 6 months, without using antibiotics in the last 6 months, and with a visual analog scale (VAS) value of sensitivity greater than 4 cm were included.
Patients with the following conditions were excluded from the study: teeth covered by prosthetics or with endodontic treatment; patients in constant use or with a medical history marked by chronic use of analgesics; anti-inflammations and psychotropic drugs; patients with orthodontic appliances; patients who have used desensitizing products in the past 3 months; patients who have undergone restorative treatment on the sensitive element in less than a month ago; removable partial denture abutment teeth; the presence of lesions with great depth (> 3 mm) who needed pulp protection; the presence of carious cervical lesion; pregnant or lactating [20].
Sample size calculation
The sample calculation was performed using the G*Power program (version 3.1.9.2 - University of Düsseldorf, Düsseldorf, Germany), based on probability distributions of the F family, with a repeated measures design, including within- and between-factor interactions. An effect size of 0.80 was obtained, measured in the between-groups comparison, resulting in 22 participants to achieve a power of 90%, with a significance level α of 5%.
DH assessment
The stimulus adopted was the evaporative stimulus (triple syringe).and tactile (probing) stimuli. The VAS with measurements from 0 to 10 was used, in which the volunteer indicated their pain. Zero (0) refers to “no pain” and 10 corresponds to “unbearable pain” [24]. The clinical evaluation involved applying a triple syringe air jet perpendicular to the cervical region of the tooth, at a distance of 1 cm. This stimulus lasted for 2 seconds. Adjacent teeth were isolated using cotton rolls to prevent any interference with the measurement of the specific tooth. Immediately following the evaporative stimulus test, the patient indicated the level of sensitivity experienced on a VAS, and this information was documented in the patient's clinical chart. The examiner responsible for assessing the level of cervical DH had undergone calibration prior to the evaluation.
All treatments were administered by the same researcher (operator 1). The stimuli and pain measurements were carried out by a previously calibrated examiner (operator 2). To minimize errors and prevent bias, operator 2, who was unaware of the treatments applied, assessed the response of each tooth to the air stimuli. Subsequently, the levels of DH were measured and recorded [25].
1. Interventions
After undergoing clinical examination and providing their consent to participate in the study, patients received treatment based on their assigned group. Two weeks prior to the start of the study, participants entered a wash-out period, during which they exclusively used oral hygiene products recommended by the researchers. These products were to be used consistently until the conclusion of the study. The oral hygiene kit included a soft toothbrush (Professional Lab Series, Colgate Palmolive Company, New York, NY, USA), a fluoride toothpaste (Colgate Total 12, 1,450 ppm F, Colgate Palmolive Company), and a dental floss (Colgate, Colgate Palmolive Company).
Prior to treatment, dental prophylaxis was conducted on all teeth using a rubber cup, 2% chlorhexidine, and a pumice stone. The area was subsequently rinsed with an air/water spray and dried using cotton. To ensure relative isolation, cotton rolls were used, and treatments were then administered based on the assigned groups. The group distribution, as well as the composition and usage instructions provided by each manufacturer, are presented in Table 1.

Description of application and composition of products used according to each manufacturer
Initially, a topical anesthetic (Benzotop 200g/mg, DFL, Rio de Janeiro, RJ, Brazil) was applied to assist in controlling any discomfort in the participants' lips for the placement of a lip retractor (Expandex White Lip Retractor, Maquira, Maringá, PR, Brazil). Participants received prophylaxis with a paste made of pumice stone (Pumice Stone, Biodinâmica, Ibiporã, PR, Brazil) and 2% chlorhexidine gluconate (Chlorhexidine Solution, Maquira), in a 1:1 ratio, using a rubber cup (Microdont, São Paulo, SP, Brazil) attached to a low-speed handpiece (Kavo, Joinville, SC, Brazil) on the teeth included in this study, followed by relative isolation using cotton rolls on the adjacent teeth. The application of all protocols was performed in a single session, and the steps of the clinical procedures are summarized in Table 2.

Description of application of management protocols
The treatments were carried out in 1 session. The effectiveness of the products was evaluated immediately after each treatment session using the VAS. Participants were scheduled for follow-up visits at 7, 30-, 60-, and 360 days post-treatment, during which the VAS level was assessed using the same evaporative and tactile stimuli.
Statistical analysis
The analysis followed the intention-to-treat protocol and involved all participants who received the management. The results were subjected to statistical analysis using JAMOVI software, version 1.2.24 (The Jamovi Project, Sydney, Australia) [26].
The data were assessed for normal distribution using the Shapiro-Wilk test, which yielded a non-normal distribution. Based on this prerequisite analysis, statistical tests were performed to evaluate the presence of statistically significant intra-group differences using the Friedman repeated measures analysis of variance (Friedman's analysis of variance [ANOVA]) followed by the Durbin-Conover post-test, with a significance level set at p < 0.05. For the analysis of data related to the degree of sensitivity among participants in the intra-group assessment, the Friedman repeated measures ANOVA was conducted, followed by the Durbin-Conover follow-up test (p < 0.05). In turn, for the inter-group analysis comparing the same time interval, the Wilcoxon test was performed (p < 0.05).
RESULTS
A total of 52 individuals were assessed for sample selection, and 28 were excluded for not meeting the inclusion criteria. In the end, 20 participants were randomized, treated, and evaluated (Figure 1).
The demographic characteristics are presented in Table 3. The mean age ranged from 19 to 60 years, with the majority being of Caucasian ethnicity and female sex.

Patient data regarding sex, race, and age
Analysis of dentin sensitivity level
The results were subjected to statistical analysis using the non-parametric Friedman repeated measures ANOVA test (p < 0.05), followed by the Durbin-Conover post hoc test (p < 0.05) for intra-group evaluation. For inter-group analysis, the Wilcoxon test (p < 0.05) was used. Overall, in most evaluations, there was no statistically significant difference between the tested desensitizing agents at different reassessment times.
The evaluation of sensitivity level generally showed a statistically significant difference between the initial time points and the other evaluated times in the intra-group analysis. Another important finding is that for the 12-month evaluation (T5), all groups showed a statistically significant difference compared to the initial evaluation. In terms of inter-group analysis, there was a statistically significant difference between the Mixed Desensitizing Protocol (PAM) group and Remineralizing Desensitizing Protocol (PDR) group at the initial evaluation (T1). For the assessment at 12 months (T5), there was a statistically significant difference between the PAM group and the control group, and PDR group. The data are presented in Table 4.

Median values and interquartile ranges of sensitivity level during the execution of the tooth whitening protocol using desensitizing agents control group, PDN group, PAM group, and PDR group at different assessment times
DISCUSSION
This study demonstrated that all protocols were effective in reducing DH. A higher incidence of DH was observed in women, which is consistent with findings from other studies [2627]. However, another study reported a higher prevalence of DH in males, with 68 out of 90 participants being affected [28]. Thus, it can be inferred that in the Brazilian context, DH predominantly affects females, unlike in other countries. The study population consistently exhibited similar baseline characteristics across all treatment groups, which aligns with a clinical study conducted by Lopes et al. [29], who also evaluated different management protocols for DH.
The results of this study provide evidence in support of the formulated hypothesis, suggesting that the application of an associative protocol using neural agents followed by obliterating agents in the same clinical session would lead to a significant reduction in DH. This hypothesis is based on the synergistic combination of the depolarizing and tubule-sealing effects provided by the agents used. The study findings confirmed this hypothesis, as a substantial reduction in hypersensitivity was observed throughout the evaluation period. Thus, the associative protocol proved to be an effective approach in managing DH.
The results of this study regarding SBU are similar to those found by other researchers. The positive effect may be related to its composition, as the chemical interaction of the dental substrate with 10-methacryloyloxydecyl dihydrogen phosphate (10-MDP) forms an MDP-Ca salt, which is responsible for improved adhesion and greater stability in an aqueous environment [29]. The reduction and control of DH occur because the protein precipitates present on the dental surface are not permeable to the monomers present in SBU's composition, and the presence of phosphorylated monomers allows for bonding with dentin when in an aqueous environment, enabling the obliteration of open tubules [30].
However, when comparing Gluma Desensitizer, Gluma Comfort Bond + Desensitizer, and SBU, the adhesive showed less effective results in controlling DH [31]. The application of a double layer of SBU in this study may have contributed to the effectiveness of sensitivity control.
A 4-session protocol for reducing DH, using Desensibilize KF 2% (FGM, Joinville, SC, Brazil), Clinpro XT Varnish, and Photo Lase III, demonstrated that Desensibilize KF 2% was effective in controlling sensitivity, as observed in this study [26]. The immediate efficacy of neural action products is attributed to the presence of potassium nitrate in their composition, which depolarizes the cells on the dental surface and in the dentinal tubules, thus preventing sensitivity [1232]. This immediate reduction efficiency was demonstrated in an in vitro study, where potassium nitrate was able to penetrate the dental pulp within 5 minutes [33].
Obliterative agents are also used in the control of DH, and in this study, Enamelast (Ultradent, South Jordan, UT, USA) was chosen, which contains sodium fluoride that deposits fluoride ions and obliterates the dentinal tubules, preventing external stimuli from causing hypersensitivity [33]. This deposition of ions on the dental surface was confirmed in an in vitro study, where Enamelast showed higher microhardness values and a higher concentration of fluoride in its composition compared to Duraphat (Colgate Palmolive Company) and Clinpro White Varnish (3M ESPE, St. Paul, MO, USA) [3435].
In this study, a mixed protocol was proposed, where the neural agent Desensibilize KF 2% was applied first, followed by the obliterative agent Enamelast. The neural agent's function is to depolarize the nerve fibers, preventing the transmission of nerve impulses, thereby controlling sensitivity. It is important to apply the correct sequence due to the mechanism of action of the agents used. If the dentinal tubule orifice is sealed before the depolarization of the nerve fibers, the desired efficacy of this protocol is compromised [123336].
By combining agents with different mechanisms of action, it is possible to achieve a more effective and long-lasting result, as these actions can interact positively. The present associative protocol demonstrated efficacy in treating DH in all evaluations, showing a reduction from the first assessment. In a previous study that used potassium oxalate, an agent with neural and obliterative properties for DH control, a significant reduction in hypersensitivity complaints was observed in all assessments [27].
The clinical study used Profluorid Varnish, Admira Protect, and PRG-Barrier Coat (PBC) for DH control, evaluated through evaporative and tactile tests immediately after, 1 week, and 1 month after the application of the agents. The study showed that all products had positive results in reducing DH at all time intervals, which differs from the results of this research where the PBC desensitizer was more effective in reducing DH after 7 days of application [15]. This discrepancy may have been caused by the difference in prophylaxis procedures, as the authors used a Robinson brush instead of a rubber cup, which was different from this study.
Similar results were found in a clinical study comparing PBC and BiFluorid 10 for reducing DH, where PBC showed a significant difference only in the evaluation conducted 1 week after application [37]. The fact that the reduction in DH does not occur immediately after the application of PBC may be related to its mechanism of action, which occurs gradually when in contact with oral fluids, by binding ions to collagen fibers, while fluoride and strontium bind to apatite present in the dental structure, improving its resistance to acid attack [22].
The results obtained in this study were significant for the management of DH at all proposed time points, and they particularly stood out in the PDR and control groups. It should be mentioned that PBC is a promising agent that has demonstrated its long-lasting effect in managing DH due to its mechanism of ion release and precipitation, aiding in remineralization and obliteration of dentinal tubules, as observed after 12 months of application in this study, as well as in the Control group [37]. This is attributed to the characteristics of SBU, with the presence of 10-MDP, which stabilizes in an aqueous medium and chemically bonds with dentin, obliterating the dentinal tubules [32].
The scarcity of clinical trials and lack of scientific evidence pose a challenge in providing precise information on the long-term clinical efficacy of materials used in the management of DH. However, the results of this study demonstrate that these materials hold promise for the treatment of DH. Further clinical trials are recommended to compare the desensitizing effect among different materials, in order to maximize their benefits and improve their utilization in clinical practice. Additionally, future studies can explore the influence of variables such as age, sex, and specific oral conditions on the effectiveness of these associative protocols, further enhancing the understanding and management of DH.
CONCLUSIONS
Based on this study, it can be concluded that all the protocols employed were effective in reducing DH from the initial evaluation, as observed within each group, up to 12 months. In the intergroup evaluation, the control and PDR groups demonstrated greater efficacy in controlling DH after 12 months.
The clinical relevance of this study is to demonstrate that the application of single-session desensitizing protocols can be effective in controlling DH for up to 12 months, as demonstrated by statistical analysis.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: Zeni TC, Cardoso PMdeF Vanolli RdaS.
Data curation: Vanolli RdaS, Mendonça MJ, Camilotti V.
Formal analysis: Cardoso PMdeF, Mendonça MJ.
Funding acquisition: Vanolli RdaS, Ueda JK Investigation.
Methodology: Mendonça MJ.
Project administration: Zeni TC.
Resources: Camilotti V.
Software: Cardoso PMdeF, Camilotti V.
Supervision: Vanolli RdaS, Validation.
Visualization: Zeni TC, Writing - original draft.
Writing - review & editing: Ueda JK, Cardoso PMdeF, Mendonça MJ Camilotti V.



