Does minimally invasive canal preparation provide higher fracture resistance of endodontically treated teeth? A systematic review of in vitro studies
Article information

Abstract
This systematic review aimed to investigate whether minimally invasive root canal preparation ensures higher fracture resistance compared to conventional root canal preparation in endodontically treated teeth (ETT). A comprehensive search strategy was conducted on the “PubMed, Web of Science, and Scopus” databases, alongside reference and hand searches, with language restrictions applied. Two independent reviews selected pertinent laboratory studies that explored the effect of minimally invasive root canal preparation on fracture resistance, in comparison to larger preparation counterparts. The quality of the studies was assessed, and the risk of bias was categorized as low, moderate, or high. The electronic search yielded a total of 1,767 articles. After applying eligibility criteria, 8 studies were included. Given the low methodological quality of these studies and the large variability of fracture resistance values, the impact of reduced apical size and/or taper on the fracture resistance of the ETT can be considered uncertain. This systematic review could not reveal sufficient evidence regarding the effect of minimally invasive preparation on increasing fracture resistance of ETT, primarily due to the inherent limitations of the studies and the moderate risk of bias.
INTRODUCTION
The primary objectives of endodontic treatments are to prevent or treat apical periodontitis and ensure the long-term survival of root-filled teeth [1]. The complete removal of bacteria and their by-products, which play a pivotal role in the development of pulpal and periapical disease, is a crucial step [2]. Since mechanical instrumentation is unable to completely touch root canal walls and remove the bacterial load, irrigation has garnered attention over the past decades [345]. However, effective mechanical remains an essential step directly associated with the success of root canal treatment. This importance stems not only from its mechanical action but also from the creation of a pathway for irrigating the root canal system [6].
There is still ongoing debate regarding the optimal apical enlargement dimension for achieving favorable outcomes. Existing literature includes several studies indicating that larger preparations result in significantly enhanced disinfection, influenced by multiple factors. Greater apical enlargement leads to a reduction in unprepared canal area, thereby more effectively eliminating biofilms and infected dentine [7891011]. Additionally, it facilitates improved irrigation flushing of the apical third, offering a larger volume, and leading to a more substantial reduction in bacterial load [111213]. Consistent with these observations, a prospective randomized clinical trial (RCT) demonstrated that apical preparations 2 sizes larger than the initial apical binding file with a 0.04 taper exhibited lower success rates compared to larger preparation sizes (e.g., 3 sizes larger than the initial apical binding file) and tapers (0.06 taper) [14]. Another randomized controlled trial also demonstrated improved outcomes associated with increasing apical preparation size [15].
In the last years, Endodontics has been moving towards minimally invasive endodontics, emphasizing the preservation of healthy dental hard tissue to uphold the tooth’s strength and integrity while preventing or treating diseases [16]. Initially centered on access cavity design and preservation of pericervical dentine, this concept has progressed to encompass minimally invasive root canal preparations [17181920]. Instruments with a reduced apical diameter and taper have been suggested in the scope of minimally invasive approaches [2122]. The primary concern associated with the use of instruments having smaller tapers and apical sizes revolves around ensuring proper cleanliness within the root canal space [623]. Previous studies indicated that smaller tapers did not significantly affect root canal cleaning [2024]. Conversely, minimal canal enlargement has also been linked to incomplete debris, smear layer, pathogenic bacteria, infected dentine, and pulp remnants removal [25262728]. Nevertheless, the debate persists regarding whether larger instrumentation sizes lead to excessive dentin removal, potentially weakening the tooth’s structure [14]. Currently, there is insufficient evidence to establish a direct correlation between a specific preparation size and fractures in endodontically treated teeth. Regarding divergent results, the fracture resistance comparisons between different tapers and apical sizes are still unclear [1929].
Based on these premises, the objective of this systematic review is to address the following question: Does the adoption of minimally invasive preparation, featuring lower apical preparation and/or taper size, result in enhanced fracture resistance in endodontically treated teeth compared to larger preparation?
MATERIALS AND METHODS
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis principles (PRISMA) (http://www.prisma-statement.org/). The study protocol was registered in the Open Science Framework (DOI No.: 10.17605/OSF.IO/CXB24).
Eligibility criteria
In vitro studies comparing the impact of at least 2 different root canal preparation sizes, in terms of apical diameter and/or taper, on fracture resistance of endodontically treated teeth were selected. There were no limitations on publication dates, and only articles published in English were considered for inclusion.
Reviews, case series, letters, animal studies, finite element analysis studies, and conference abstracts were not included. The eligibility criteria were established according to the Population, Intervention, Comparison, Outcome, and Study design (PICOS) strategy, as follows:
Population (P): Extracted human teeth with fully formed (mature) apex;
Intervention (I): Minimally invasive preparation;
Comparison (C): Larger preparation;
Outcome (O): Fracture resistance; and
Study design (S): In vitro studies.
Database selection and searching strategy
This systematic review focused on evaluating the impact of minimally invasive preparation on the fracture resistance of endodontically treated teeth compared to the larger apical size and/or taper counterparts. Two independent reviewers performed the ultimate search using “PubMed (MEDLINE), Web of Science (all databases), and Scopus” databases as shown in Table 1. Researchers with experience in endodontics and/or systematic review designed the terms and search strategy. The related keywords with minimally invasive preparation, fracture resistance, and endodontics were chosen and enhanced during the search process. Additionally, a hand search was conducted in the Journal of Endodontics and the International Endodontic Journal in order to identify any related article that could not be recovered through electronic search.

Search strategies and obtained article numbers from databases
Selection of the studies
After the searching process was completed, the collected articles were exported and compiled in Microsoft Excel software to eliminate duplicates and enhance manageability. Two independent reviewers (SNU and SF) assessed the titles and abstracts of selected articles. The full text was accessed if the title or abstract did not give adequate information for the inclusion or exclusion of the study. Secondly, full texts of articles were read to determine whether the relevant studies would be included based on the eligibility criteria by the same 2 reviewers. Studies involving finite element analyses and those employing separated root segments were excluded. Disagreements between the reviewers were discussed until a consensus was reached. In cases of persistent disagreements, a third reviewer (EJNLS) was consulted for resolution. Following the comprehensive full-text assessment, pertinent studies related to the topic were incorporated into this systematic review.
Data extraction
Two reviewers (SNU and SF) independently extracted the data from the selected studies to summarize each study, and the results were recorded. All pertinent indicators that could influence the study’s outcomes were identified and documented. This included details such as study characteristics (authors, publication year, and country), sample characteristics (tooth type and group sample size), specifics of the endodontic procedures (apical size and taper, filling, restoration), fracture strength (load at fracture test), and primary results. Any disagreements were resolved again by consulting other reviewers (EJNLS and MG).
Risk of bias
A risk of bias analysis was carried out for the selected studies. In this sense, evaluation methods were adapted to the ones used in previous systematic reviews concerning in vitro studies [303132]. The same 2 reviewers examined the methodological quality of each selected study independently according to the following parameters: sample size calculation, samples with similar dimensions, application of root canal filling procedures, presence of coronal restoration, and proper statistical analysis. If the parameters were reported in the study, ‘YES’ was assigned, and ‘NO’ was assigned if the parameters could not be reported. The risk of bias was classified according to the number of ‘YES’ as high (1 or 2 parameters), moderate (3, 4), and low (5 or 6 parameters).
The objective of determining the appropriate sample size is to ensure that studies can effectively identify clinically significant differences [33]. Study power was assessed based on the average fracture resistance, standard deviations, and sample sizes for each tooth group. The power calculation was performed using G*Power software (G*Power 3.1.9.4, Heinrich-Heine, Dusseldorf, Germany). Firstly, the effect sizes were calculated using 1-way fixed effects analysis of variance (ANOVA) test with %95 power. Subsequently, study powers were computed through post-hoc analysis at a significance level of 0.05.
Review
A total of 1,767 articles were identified through the electronic search: 608 from PubMed, 194 from Web of Science, and 965 from Scopus. After applying the eligibility criteria and discarding the duplicates, 14 articles were selected for full-text assessment. Subsequently, these articles were read completely, and 6 were excluded since they were finite element analyses or separated the root segment (Figure 1). As a result, 8 studies fulfilled the eligibility criteria and were included in this systematic review [3435363738394041].
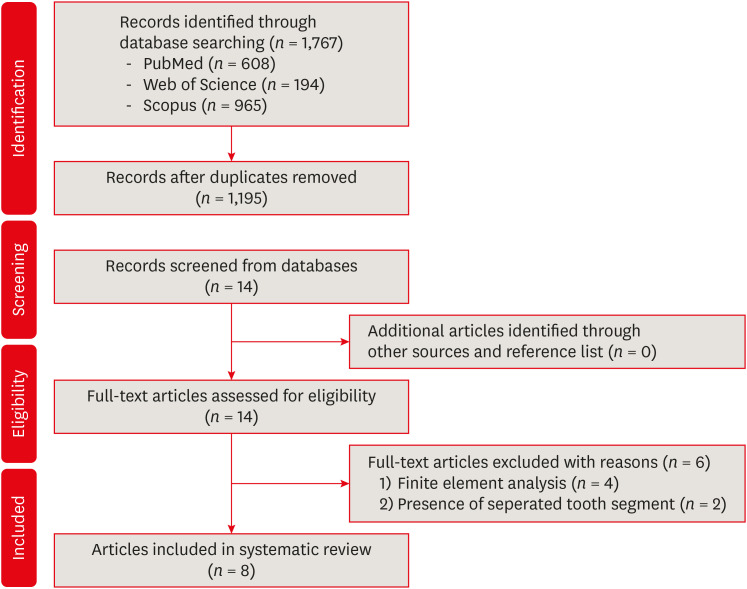
Flow diagram of the searching strategy process.
Study characteristics
All the included studies focused on investigating the influence of apical preparation size and/or taper on the fracture resistance of extracted human teeth. These studies examined a range of tooth types, including maxillary premolars, mandibular incisors, premolars, and molars [3435363738394041]. Notably, the sample size per group exhibited variations, ranging from 8 to 30 [3640]. Prior to conducting the fracture resistance tests, some studies did not perform root canal filling or restoration procedures [343537383941]. Moreover, dissimilarities were observed in the methodologies employed for fracture resistance testing. While Augusto et al. [40] conducted tests at a 30° angle to simulate clinical conditions, the other authors applied vertical loads parallel to the long axis. The crosshead diameter varied across studies, with a testing speed of 1 mm/min, except for 1 study that used a speed of 0.5 mm/min [38]. The studies also exhibited considerable diversity in the fracture resistance values and standard deviations.
Fracture resistance results of studies
Table 2 presents the characteristic details of the included studies along with their main statistical findings. Çapar et al. [34] reported no statistically significant differences among the tested groups. Çiçek et al. [35] revealed a statistically significant difference between ProTaper Next (X4, 40/0.06) and Mtwo (40/0.06). Moreover, the resistance to vertical root fracture was comparable between the WaveOne reciprocating file (40/.08v) and Revo-S (AS, 40/0.06), while the Twisted File (40/0.04) exhibited lower resistance compared to other groups. Zogheib et al. [36] observed no statistically significant difference between the 0.04 and 0.06 taper preparations in maxillary premolars. Krikeli et al. [37] indicated that different tapers did not yield statistically significant differences between experimental groups. Tian et al. [38] demonstrated that the 40/0.05 group had higher fracture resistance than the 55/0.05, 60/0.05, and 45/0.15 groups. They also noted a statistically significant difference between the 45/0.05 and 45/0.15 groups. Doğanay Yıldız et al. [39] assessed mandibular incisors for fracture resistance and found that altering the taper from 0.04 to 0.06 or from 0.06 to 0.08 without changing apical preparation size did not result in statistically significant differences. Augusto et al. [40] investigated load fracture in different access cavities and taper preparations in mandibular molars, and no significant differences in fracture resistance were observed among the tested groups. Lin et al. [41] reported that root canal-treated mandibular premolars instrumented with 0.04 taper NiTi rotary files exhibited higher fracture resistance than those with 0.06 tapers.

Summary of the main characteristics and results of the included studies
Risk of bias and the power analysis assessment
Two studies demonstrated a low risk of bias, while 6 studies exhibited a moderate risk of bias. The results are presented in Table 3 according to the determined parameters in the review [4041].

Risk of bias of the included studies
The power analysis for the included studies is outlined in Table 4. The power analysis indicated some studies with a high power ranging from 86.19% to 100% [3738]. Meanwhile, studies with low power ranged from 15.11% to 77.47% [3641].

Power analysis assessment of included studies
DISCUSSION
The overarching purpose of endodontic treatment is to prevent and treat apical periodontitis by effectively removing bacteria and related by-products from the root canal space through proper chemomechanical debridement [5]. The concept of canal preparation highlights the importance of achieving an appropriate enlargement size to allow optimal disinfection [42]. However, there exists no consensus in the literature regarding the optimal size of enlargement for achieving improved treatment outcomes, largely due to the limited number of RCTs addressing this contentious issue [15]. Previous studies have demonstrated a positive correlation between larger preparations and enhanced disinfection [943]. Nevertheless, using instruments with high tapers and apical sizes could potentially result in increased removal of dentin, raising concerns about the possibility of root fractures [34]. In this sense, instruments with reduced tapers and sizes have been suggested to preserve more dentine and reduce stress, particularly in the coronal third of the root [44]. Guided by this background information, the primary objective of this systematic review was to assess whether root canal preparation using instruments with reduced tapers and/or apical sizes yields higher fracture resistance in endodontically treated teeth.
Eight of 1,767 studies recovered from 3 databases were included in this systematic review after the eligibility criteria and removing duplicates. Given the diversity in instrumentation systems, selected teeth, and methodologies among the studies, a meta-analysis is not advisable. In 3 studies included in this review, groups using instruments with reduced tapers demonstrated higher fracture resistance values, regardless of the apical size [383941]. However, fracture resistance values did not exhibit statistically significant differences in the other 5 included studies. For instance, Tian et al. [38] identified a notable difference in fracture resistance between 0.05 and 0.15 tapers with the same apical size, accompanied by a moderate risk of bias. Another study with a moderate risk of bias performed by Doğanay Yıldız et al. [39] observed a significant difference when increasing the taper from .04 to .08. These findings could potentially be attributed to greater variations in the tested tapers (for e.g., 0.05 vs. 0.15, and 0.04 vs. 0.08) and the absence of coronal restorations. Interestingly, Lin et al. [41] found a significant difference between 0.04 and 0.06 tapers with a low risk of bias. The heterogeneity of outcomes may be linked to multiple factors. The utilization of various file systems with distinct designs, kinematics, and rotational speed and torque values in the studies introduces the possibility of impacting the mechanical structure of dentin at varying rates, thereby posing challenges to direct study comparisons.
Tooth type and root canal anatomy are additional factors influencing fracture resistance. Molar teeth, for instance, possess a greater amount of structure on the pulp chamber floor compared to the premolars and incisors, potentially contributing to heightened fracture strength. Additionally, the curvature of the external root surface plays a pivotal role in stress distribution, impacting both susceptibility and pattern of fracture [45]. It has been suggested that an increased degree of root curvature leads to a greater volume or area of stress concentration within the root dentin [46]. In the scope of this review, each study maintained internal standardization, considering anatomical and morphological traits of the teeth with similar dimensions and straight or low-curved root canals. This approach enhances result reliability within each study. However, when comparing the different studies, it is important to acknowledge that anatomical and morphological diversities of the teeth used can introduce confounding factors, potentially complicating the accurate interpretation of results.
Endodontically treated teeth respond to occlusal forces in distinct ways, shaped by their morphological attributes, remaining coronal surface structures, and locations [47]. Consequently, preserving the coronal aspect or simulating its restoration becomes pivotal, not only to replicate real clinical scenarios but also to bolster the reliability of fracture tests. In this systematic review, only 2 studies preserved the entire tooth integrity and stated no significant difference between the tested groups regarding fracture resistance [3640]. This can be explained by the fact that the reconstruction of endodontically treated teeth with suitable coronal restoration could enhance the biomechanical behavior by minimalizing the stress transmission to the root [48]. In contrast, the other 6 studies subjected decoronated teeth to fracture tests. Decoronation of teeth may jeopardize the achievement of accurate fracture resistance values, as it excludes weakening of the crown structure after endodontic treatments [49]. Coincidentally, all studies that demonstrated differences between the different types of root canal preparation did not perform coronal restoration [383941]. Since previous research has indicated that restored teeth can regain up to 72% of their fracture resistance compared to untreated teeth the absence of coronal restoration in these particular studies might influence the impact of different preparation sizes on fracture resistance [17]. Given the undeniable influence of coronal structures on fracture resistance values, it's prudent to interpret the outcomes of these studies with caution. Additionally, some studies have reported that root canal filling can increase fracture resistance values due to bonding at the dentin-sealer interface, which acts as a stress dispersal [5051]. Except for 2 studies in this review, root canals were filled with gutta-percha and sealer before the fracture test [3839].
Although well-designed in vitro studies could also contribute to clinical problems and guide future research by defining the lack of present studies and revealing their limitations, it is obvious that in vitro studies cannot simulate oral clinical conditions, and thus, it is difficult to make inferences directly about clinical applications [52]. In this sense, when seeking answers to specific questions, RCTs provide the most reliable evidence [53]. However, performing clinical research requires a workforce and costs; therefore, it needs to be conducted cost-benefit analysis before being carried out [3154]. The included studies were insufficient to demonstrate the in vitro benefit of the minimally invasive preparation in the concept of this systematic review.
The heterogeneity of the included studies makes it difficult to guide the results to draw a summary conclusion. When interpreting the findings, it’s crucial to consider variables like tooth types, methodologies, and file systems, as these factors significantly influence the outcomes. Such aspects of standardization and randomization would enhance the quality of results. Given the variance in biases observed, this systematic review was unable to provide substantial evidence regarding the effects of minimally invasive preparation on enhancing the fracture resistance of endodontically treated teeth. Despite these limitations, this systematic review serves as a valuable stepping stone for understanding the relationship between minimally invasive preparation and fracture resistance in endodontically treated teeth. Further research endeavors, encompassing rigorous study designs, enhanced standardization, and a closer alignment with clinical realities, are required to provide a more comprehensive and conclusive understanding of this intricate interaction. As the field of endodontics continues to evolve, addressing these limitations will undoubtedly contribute to refining our insights into the impact of minimally invasive approaches on the biomechanical integrity of endodontically treated teeth.
CONCLUSIONS
The heterogeneity of available data, stemming from low-quality studies with a moderate risk of bias, impedes a definitive determination on whether minimally invasive root canal preparation guarantees higher fracture resistance compared to conventional root canal preparation for endodontically treated teeth. The current body of evidence lacks the robustness required to ascertain the long-term implications of minimally invasive root canal preparations on treatment outcomes. Consequently, this systematic review remains inconclusive in revealing substantial evidence concerning the impact of minimally invasive preparation in augmenting fracture resistance of endodontically treated teeth.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: Usta SN, Silva EJNL, Gündoğar M.
Data curation: Usta SN, Falakaloğlu S.
Formal analysis: Usta SN.
Investigation: Usta SN, Silva EJNL, Falakaloğlu S.
Methodology: Usta SN, Silva EJNL.
Software: Usta SN, Falakaloğlu S.
Supervision: Silva EJNL, Gündoğar M.
Validation: Usta SN, Silva EJNL, Falakaloğlu S, Gündoğar M.
Visualization: Usta SN, Silva EJNL, Falakaloğlu S, Gündoğar M.
Writing - original draft: Usta SN, Silva EJNL.
Writing - review & editing: Usta SN, Silva EJNL, Falakaloğlu S, Gündoğar M.



