Ingestion and surgical retrieval of an endodontic file: a case report
Article information

Abstract
Ingestions and aspirations of foreign bodies are rare, but do occasionally occur during dental treatment. Although reports exist, few include photos demonstrating the extensive surgical intervention that may be necessary to manage such events. Perhaps this lack of visualization, and associated lack of awareness, is one of the reasons some clinicians still provide non-surgical root canal therapy (NSRCT) without a rubber dam. This case report outlines the medical treatment of a 30-year-old male who initially presented to a general dentist’s office (not associated with the authors) for NSRCT of their mandibular right first molar. A rubber dam was not used for this procedure, during which the accidental ingestion of an endodontic K-file occurred. The patient was subsequently hospitalized for evaluation and treatment, consisting of numerous imaging studies, endoscopic evaluation, and surgical removal of the file from his small intestine. The ingestion of foreign bodies, and the associated complications, can be reduced through the routine use of a rubber dam, which is considered the standard of care for NSRCT. This case graphically illustrates the potential consequences associated with deviating from the standard of care and should remind clinicians that a rubber dam is necessary for all cases of NSRCT.
INTRODUCTION
For non-surgical root canal therapy (NSRCT), the use of a rubber dam is considered the standard of care [1]. Its use has been shown to aid in the creation of an aseptic operating field, thereby improving infection control and increasing treatment efficacy, while also helping to protect the patient from ingesting solutions and foreign bodies [2].
Ingestions and aspirations of foreign bodies are rare, but do occasionally occur during dental treatment. It is estimated that the ingestion of endodontic instrument(s) occurs at an incidence of 0.12 per 100,000 root canal treatments. Aspirations are reported less frequently, with an incidence of 0.001 per 100,000 root canal treatments [3].
When a foreign body is ingested, approximately 13% will enter the respiratory tract and 87% will enter the gastrointestinal (GI) tract [4]. Although the majority of objects will pass through the GI tract without issue, complications such as impaction, perforation, or obstruction may occur [5]. For reasons such as these, either surgical (≤ 1% of cases) or nonsurgical (10-20% of cases) intervention to remove the object from the GI tract may be necessary [6]. Even under ideal circumstances, accidents can occur. However, preventive measures, such as a rubber dam, should still be used to reduce the frequency of ingesting foreign objects.
Although reports of accidental foreign body ingestions exist, few have been able to follow the patient’s medical journey closely enough to capture photos demonstrating how extensive the surgical intervention necessary to manage such events may be. Perhaps increasing the visualization of such events would increase awareness about the potentially life-threatening consequences associated with deviating from the standard of care in endodontics: rubber dam use during NSRCT. Currently, despite the numerous benefits, dentists frequently choose to forgo the use of a rubber dam during NSRCT [78]. It is estimated that approximately 15% of endodontists and over 50% of general dentists perform NSRCT without a rubber dam [89]. Those not using a rubber dam have cited many reasons, perhaps an additional reason is a lack of awareness about the severity of potential consequences, which may include patients needing hospitalization and/or surgical intervention [10].
This paper outlines a case of endodontic file ingestion requiring surgical management. This case serves as a graphic reminder to all clinicians performing endodontic treatment that a rubber dam is necessary for NSRCT and the potentially life-threatening consequences of deviating from this standard of care.
CASE REPORT
This case report was prepared according to the PRICE 2020 Guidelines. Informed consent for this case report was obtained for this case prior to the submission of this study [11].
A 30-year-old male presented to his general dentist’s office (not affiliated with the authors of this study) for NSRCT of their mandibular right first molar. A rubber dam was not used for this procedure, during which an endodontic file became dislodged from the tooth and was subsequently swallowed. As the patient did not have any trouble swallowing or breathing after the ingestion, the patient reported that immediate retrieval techniques, such as the Heimlich maneuver, were not attempted. A visual search of the oral cavity was conducted. When the file could not be located, the patient was immediately referred to the nearest hospital emergency department for medical evaluation and management.
Upon arrival at the hospital, a kidney, ureter and bladder (KUB) radiograph was taken (Figure 1A), revealing the presence of the file in the distal part of the stomach, approximating the outlet to the small bowel. At this time, the decision was made to move forward with an endoscopy of the upper GI tract. The endoscopy was completed without complications or abnormal findings. However, since the file could not be visualized during the procedure, the patient was admitted to the hospital for in-patient observation, which included an abdominal computed tomography (CT) scan (Figure 2) and repeated (daily) KUB radiographs (Figure 1B and 1C).
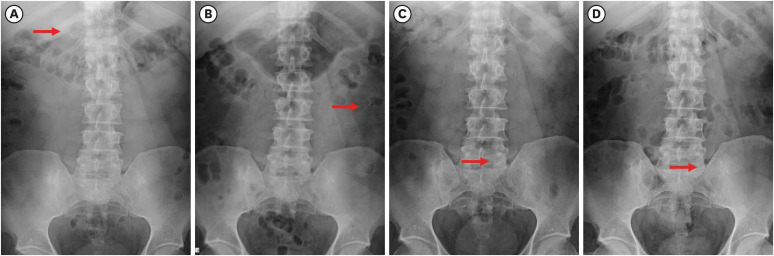
Radiographic progression of the ingested file (days 1-4). (A-C) KUB radiographs depicting the daily progression of the ingested file (red arrow) over the first 3 days of the patient’s hospitalization and (D) confirming the lack of advancement on day 4.
KUB, kidney, ureter and bladder.
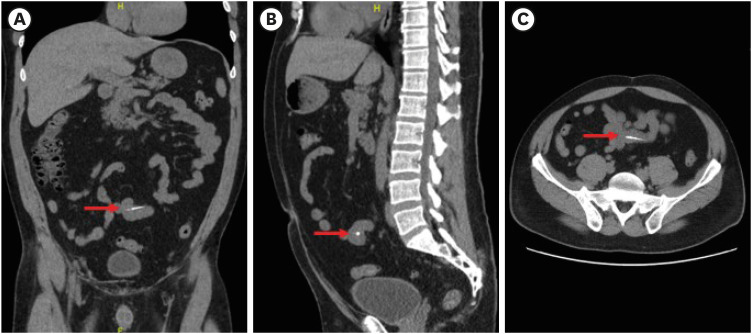
CT scan pinpointing the files halted location. (A-C) Slices from the computed tomography scan taken on day 3, locating the ingested file (red arrow) within the patient’s small intestine.
CT, computed tomography.
After 3 days of hospital monitoring, it became apparent that the file had stopped progressing (Figure 1D), and it was determined that a surgical procedure would be necessary to remove the file. The patient underwent an exploratory laparotomy (Figure 3) the following morning (Day 4). The laparoscopy revealed a 25 mm size 10 K-file assumed to be associated with an extra-abdominal adhesion. After detachment, the file was successfully removed from the small intestine, and the procedure was completed without issue. Following the procedure, the patient experienced minor post-operative sequela (bloating, etc.) from the surgery which extended his inpatient stay by 3 days. After 1 week (Day 7), the patient had sufficiently recovered and was released from the hospital. Valid informed consent, for the use of his radiographs and clinical photos, was provided by the patient prior to him leaving the hospital. The status of his endodontic treatment is unknown.
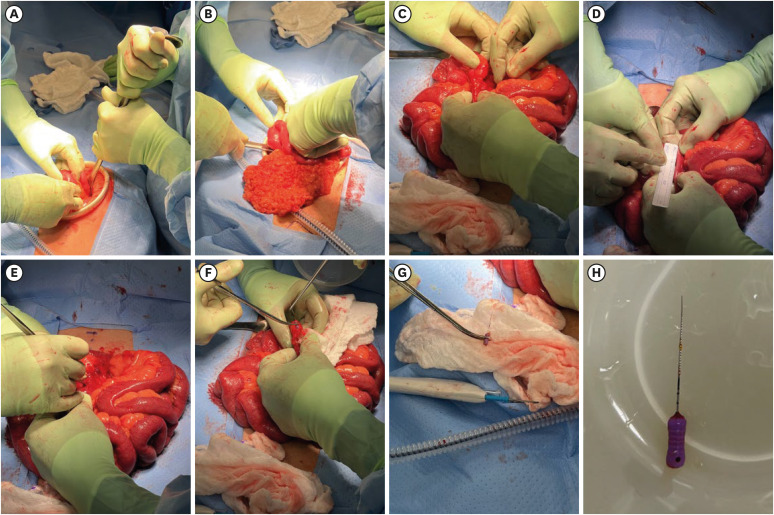
Surgical retrieval of the ingested file. (A, B) Photographs from the patient’s surgery showing the abdominal incision, tissue resection and (C, D) examination of the small intestine which contained the ingested file prior to (E, F) its removal. (G, H) Additional photographs display the retrieved file.
DISCUSSION
Previous reports have shown that, although it is uncommon, ingestions and aspirations of foreign bodies do occur during dental treatment [3512131415161718]. Since these scenarios are not ideal for the patient, nor the provider involved, preventive measures (ex. throat packs, patient positioning, etc.) should be used to help further reduce the frequency of these events during dental treatment [13]. In Endodontics, a rubber dam is likely the best tool for preventing ingestions or aspirations of foreign bodies and solutions [1319].
For NSRCT, the use of a rubber dam is considered the standard of care [1]. Its use has been shown to reduce cross-infection, improve treatment outcomes, and help protect against the ingestion or aspiration of dental materials, irrigants, and instruments [1210]. Subsequently, it safeguards providers from medico-legal issues should accidental ingestion or aspiration occur [2021]. For these reasons, the use of rubber dams during NSRCT is, almost universally, taught in dental schools and recommended by professional organizations [10].
Despite its numerous benefits, dentists frequently choose to forgo the use of a rubber dam during NSRCT [78]. Commonly cited reasons for this include a perceived lack of patient acceptance, additional time for rubber dam application, and difficulty of use [10]. However, the literature generally disputes the validity of these claims. Studies have shown that patients are generally not averse to the use of a rubber dam [10]. On the contrary, patients often report that they prefer a rubber dam to be used during treatment [10]. Furthermore, the literature suggests that even relatively inexperienced providers are typically able to place a rubber dam within minutes [10]. After initial placement, plastic frames allow for the rubber dam to remain in place during the entire procedure, without obstructing radiographic imaging [1013]. Any time “lost” during rubber dam placement is recouped by the improved working conditions afforded by the rubber dam [10]. With the rubber dam in place, providers are able to work more efficiently, without the worry of the patient’s tongue, salivary contamination, the need to change cotton rolls, or remove debris from the patient’s mouth [10]. Another potential reason is a lack of awareness about the potentially life-threatening consequences of not using a rubber dam, which may include instrument ingestion leading to patients needing hospitalization and/or surgical intervention [10].
The universal use of a rubber dam during NSRCT would greatly improve endodontic treatment and help avoid cases of accidental ingestions, such as the one outlined in this report. However, even under ideal circumstances accidents can occur. For example, rubber dam clamps can become dislodged or break during treatment, reducing the effectiveness of the rubber dam and increasing the risk of foreign body ingestion [22]. To further reduce the potential for a foreign body or clamp ingestion, some authors have suggested that dental floss should be secured to rubber dam clamps [1623]. This may allow for better location and retrieval of the clamp in the case of accidental dislodgement.
Any object (burs, endodontic files, rubber dam clamps, etc.) that becomes dislodged during treatment should be immediately retrieved and examined for potentially missing components. If the object has been accidentally swallowed and is not retrievable with hemostats or high vacuum suction, the provider may attempt to dislodge the object by placing the patient in a Reverse Trendelenburg position and encouraging the patient to cough [12]. In cases where airway obstruction occurs, the provider should also attempt to re-establish the airway with repeated back blows and/or the use of the Heimlich maneuver [524]. Emergency medical services should be contacted as needed based on the patient’s symptoms.
If an object cannot be located and confirmed to be intact, the patient must be immediately referred to a medical emergency department for further clinical and radiographic examination [1324]. Additional imaging, such as chest/abdominal radiographs, will be performed to identify the location of the swallowed object and help determine the course of medical management [24]. Approximately 13% of accidentally swallowed objects will enter the respiratory tract, necessitating the use of bronchoscopy or other surgical procedures to retrieve the object [424]. However, most objects will enter the gastrointestinal tract and will pass uneventfully without the need for intervention [4614].
Although the majority of objects will pass through the GI tract without issue, the risk for complications such as impaction, perforation, or obstruction still exists [56]. Sharp instruments, such as endodontic files, may have a higher risk of complication [25]. Therefore, strict monitoring protocols, often including serial radiographic surveillance, are put in place for these patients [1524]. If the object’s progression through the gastrointestinal tract appears stalled or the object does not pass within a reasonable amount of time (typically within 2 weeks) endoscopic retrieval or surgical intervention may be indicated [142426]. This is especially true in the case of sharp objects, such as endodontic files, whose progression through the small intestine has halted. This situation poses a significant risk for intestinal perforation and requires intervention, as was agreed upon by 2 attending physicians overseeing this case. Cases requiring surgical intervention, such as the one outlined in this report, are rare. Only 1% or less of accidental ingestions will require surgical removal [6]. When events like these occur, they do so at a significant cost to the patient, provider, and healthcare system, not only monetarily but also in terms of lost productivity, recovery time, and emotional distress.
It is the authors’ opinion that, perhaps due to a lack of collaboration between medical and dental teams, previous reports have not been able to demonstrate the severity and extent of the interventions necessary to manage such events. A strength of this case report is the close collaboration between medical and dental professionals, which allowed for real-time documentation of the patient’s condition, and, with the patients’ consent, clinical photography of the surgical intervention. Along with this case report, these photos serve as a clear example that can be used when discussing the importance of rubber dam use with our dental colleagues. Hopefully, the visualization of this information and a clear explanation of the associated consequences can help reduce the percentage of providers who perform NSRCT without a rubber dam, approximately 15% of endodontists and > 50% of general dentists, to none [89].
CONCLUSIONS
Dentists should be aware of how to appropriately manage such situations, as early diagnosis and treatment are critical to minimizing the negative sequela associated with accidental ingestions and aspirations. Furthermore, since preventive measures, such as the use of a rubber dam, can greatly reduce the frequency of these adverse events and improve the overall delivery of non-surgical endodontic treatment, continued efforts should be made to emphasize the use of rubber dams during NSRCT. Through clinical radiographs and intra-operative photos, this case graphically illustrates the potential severity of untoward events associated with deviating from the standard of care in endodontics and should serve as an example to remind all clinicians performing endodontic treatment that a rubber dam is necessary for all cases of NSRCT. This case report, and the associated images, may be used as a visual aid when discussing the importance of rubber dam usage with our dental colleagues.
ACKNOWLEDGEMENTS
The authors would like to thank Janeane Avery for her thorough review of this manuscript. The authors would like to acknowledge that this work was not funded and was carried out independently.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: Ptak DM.
Data curation: Ptak DM.
Formal analysis: Ptak DM.
Investigation: Velasquez A.
Project administration: Ptak DM.
Resources: Velasquez A.
Software: Velasquez A.
Supervision: Alon E, Amato RB.
Visualization: Ptak DM.
Writing - original draft: Ptak DM.
Writing - review & editing: Alon E, Amato RB.