The clinical success of ART restorations and Hall technique in primary molars: a randomized 18-month follow-up study
Article information

Abstract
Objectives
The aim of the study was to evaluate the clinical and radiographic success of the Hall technique (HT) and atraumatic restorative treatment (ART) restorations using high-viscosity glass-ionomer cement for the management of occlusal carious lesions in primary molars.
Materials and Methods
This randomized clinical study observed 40 children (aged 5–6 years). For each child, one tooth was treated with HT and one with ART. The primary outcome measures for HT restorations were successful, minor, and major failure rates. Clinical evaluations of ART restorations were performed according to the modified United States Public Health Service criteria during 18-month follow-up. McNemar test was used for statistical analysis.
Results
Thirty of 40 (75%) participants returned for 18 months of follow-up. In the clinical evaluations of teeth that were treated with HT, the patients did not have complaints of pain or other symptoms, all crowns remained in the oral cavity, the gums were healthy, and the teeth were functional in all evaluations. At the end of the 18-month follow-up, the surface texture and marginal integrity criteria of ART restorations were recorded as 26.7% and 33.3%, respectively. In the radiographic evaluation of 30 patients treated with ART and HT, all restorations were considered successful.
Conclusions
The 18-month clinical and radiographic results after treatments applied to single-surface cavities in anxious children showed that both treatment methods were successful.
INTRODUCTION
In the ideal treatment of primary tooth caries, dental professionals aim to protect the vitality of teeth and to ensure their maintenance in the oral cavity asymptomatically until exfoliation. Today, minimally invasive and biological treatment approaches rather than conventional restorative approaches in which the tooth is restored by completely removing carious lesions have become prominent in the treatment of primary teeth as well as permanent teeth [1]. In such techniques, the complete elimination of the cariogenic biofilm, which is the main etiological factor in caries formation, and supporting remineralization with fluoride have been adopted [2].
Primary molars are the teeth with the highest caries tendency among primary teeth due to their wide and smooth interface surfaces [3]. However, some difficulties are encountered during the removal of carious tissue in children due to reasons such as the anatomical and histological structures of the primary molars and the young age of the patients. For this reason, techniques beyond the conventional approaches to treating these teeth have come to the fore. Atraumatic restorative treatment (ART), in which the soft caries lesion is cleaned with the help of a sharp hand instrument and restored with glass ionomer cement (GIC), which releases fluoride and has adhesive properties, was introduced in 1985, followed by Hall technique (HT), which is a minimally invasive biological approach in which stainless steel crowns (SSCs) are placed without caries removal, local anesthesia, and tooth preparation [24].
The ART technique, which has begun to be applied in cases in which optimal clinical conditions cannot be provided, is a proven method to use when children do not allow treatment with conventional methods. In this treatment method, more healthy dental tissue is preserved compared to the conventional approach and dental fear in pediatric patients can be minimized [156]. Several restorative materials, especially GIC, have been utilized for ART procedures, and with advances in technology, high-viscosity glass-ionomer cements (HVGICs) with improved mechanical and chemical properties have emerged. In recent years, zinc-added HVGICs and nano-filled resin-modified HVGICs have also been marketed [7].
The HT is recommended in the treatment of asymptomatic decayed primary molars in anxious and fearful pediatric patients to ensure cooperation during treatment [4]. This technique, which does not require caries removal and tooth preparation, aims to stop the progression of caries by covering the primary molars with SSC and eliminating their relationship with the oral environment [8]. Because the bacteria can no longer use carbohydrates in the oral environment, the amount of bacteria decreases.
Studies conducted with HT and ART have reported that restorations with either technique are successful in primary molars [6891011]. However, more long-term clinical studies are needed to examine the success of these techniques in the treatment of carious lesions on different surfaces of the teeth and different layers of dentin, to determine the applicability of ART in children who cannot be treated with HT, and to support the incorporation of these techniques into routine usage.
The present study aimed to evaluate the clinical and radiographic outcomes of ART restorations with HVGIC and restorations with HT in primary molar occlusal caries lesions with 5–6-year-old children over 18 months.
MATERIALS AND METHODS
This randomized controlled split-mouth design clinical trial was conducted in the Department of Pediatric Dentistry of Faculty of Dentistry, Suleyman Demirel University. The required ethical approval for this study was obtained from the Clinical Research Ethics Committee of the Faculty of Medicine, Suleyman Demirel University (2014/157) according to the principles of the Declaration of Helsinki and has been registered in ClinicalTrials.gov (NCT05462808). The Consolidated Standards of Reporting Trials guideline was followed.
Sample size
Sample size calculation was performed using G*Power (v 3.0.1, Franz Faul, Universität Kiel, Germany). The significance level was set at 0.05, and a power of 0.80 was used. The final sample size was determined to be a total of minimum of 30 patients. Considering the dropouts in the follow-ups, the number of participants was determined as 40.
Eligibility criteria
The study population comprised children aged from 5 to 6 attending the Department of Pediatric Dentistry for routine control and dental treatment. The inclusion criteria for participants were children: (1) with no systemic disease, (2) with a score of 2 on the Frankl behavioral scale, (3) with no occlusal problems or bad habits, (4) presenting with between 2 and 5 caries lesions in primary molars, and (5) with no extracted primary molars [12]. The clinical inclusion criteria for teeth were: clinically, (1) teeth with occlusal surface caries, (2) in occlusion with the antagonist tooth/teeth, (3) in contact with the neighboring tooth/teeth, (4) teeth with no developmental anomalies, and (5) absence of spontaneous pain and tenderness to percussion; radiographically, (1) dentin caries on the occlusal surface (score 3), (2) presence of permanent tooth germ, (3) no alveolar bone destruction, (4) presence of any radiolucent in furcation and/or periradicular regions, (5) no pathological and internal/external resorption [13].
Randomization
Parents of children were informed about the treatment techniques before treatments. Written informed consent was obtained from all parents who agreed to have their children participate in the study.
All participants who met the eligibility criteria were randomly divided into 2 groups: (1) ART restorations with HVGIC and (2) Restorations with HT. To decide which of the selected teeth in the same child should receive HT or ART, the patient was asked to choose 1 of 2 cards with numbers on them, and randomization was achieved by applying the technique corresponding to that number.
Treatment procedure
Before starting the treatment, digital photographs of the teeth to be restored were taken and recorded. All treatments were performed by a trained pediatric dentist (C.K) and carried out according to the standard protocols [214]. All primary molars were treated without local anesthesia and tooth preparation. Isolation was achieved using a saliva ejector and cotton rolls.
In the HT group, the debris on the occlusal surface of the teeth was gently removed, and an appropriate size SSC (3M ESPE, St. Paul, MN, USA) was placed and cemented using GIC (Ketac Molar, 3M ESPE, Seefeld, Germany) which was prepared according to the manufacturer’s instruction. The crown was pressed tightly on the tooth by the dentist’s finger pressure, the crown position was checked, the patient bit on a cotton roll, and the crown was fully seated. Then, the excess GIC was removed quickly. Soft demineralized carious tissue was removed with a sharp excavator (153/154, Henry Schein, Melville, NY, USA) in the same patient’s other primary molar that was restored with encapsulated EQUIA Forte (GC Corp., Leuven, Belgium) according to ART protocol [2]. Each capsule of EQUIA Forte was mixed for 10 seconds. Under cotton roll isolation, teeth were restored with EQUIA Forte cement. After the setting of cement, excess material was removed with an excavator and carver instrument. The occlusion was checked for interferences by using carbon paper. A layer of EQUIA Forte Coat (GC Corp.) was applied on the surface and then light-cured for 20 seconds (Figure 1).
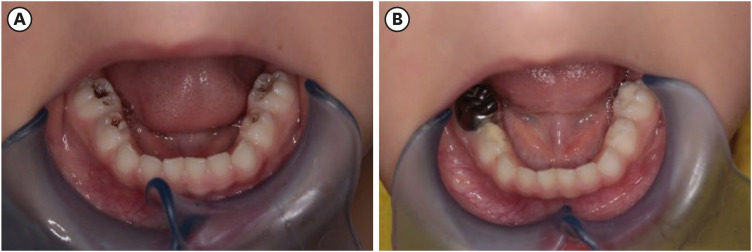
Clinical images of Hall technique and atraumatic restorative treatment restorations. (A) Before treatment. (B) Baseline treatment.
After the treatment, children/parents were informed about brushing on a model, oral hygiene motivation training, and dietary guidance were given. Participants with other dental needs were treated by the same pediatric dentist (C.K). The parents were informed that if their children had any complaints during the follow-up period, it was necessary to contact the physician immediately.
Follow-up
Photographs of the selected teeth were taken immediately after treatment and at 6, 12, and 18 months after treatment. All treated teeth were evaluated clinically at 3-month intervals and radiographically at 6-month intervals.
For clinical evaluation, a mouth mirror and an explorer were used under reflector light. Clinical evaluations of ART restorations using EQUIA Forte were performed according to the modified United States Public Health Service (USPHS) criteria (anatomic form, surface texture, marginal discoloration, color match, marginal integrity, secondary caries, and retention) [15]. The restorations were scored as Alpha (A), clinically ideal “successful”; Bravo (B), clinically “acceptable”; Charlie (C), clinically unacceptable “unsuccessful” restorations. Outcome criteria for assessment of HT restorations were made according to Innes et al. [16] (Table 1). HT treatments scored as satisfactory were considered “successful,” while those with minor and/or major failures were considered as “failed.” We also asked patients about their satisfaction with the restorations at the follow-up intervals after treatment.

Statistical analysis
The data were entered in SPSS version 23.0 for Windows (IBM Corporation, Armonk, NY, USA). ART restorations evaluated according to USPHS criteria were compared over time using McNemar's test. Statistical significance was set at p < 0.05.
RESULTS
During the study period, 40 children received restorations with HT and ART. After excluding 10 patients who did not attend the follow-up intervals due to reasons such as family migration and no response to phone calls, 60 teeth of 30 treated patients (mean age: 5.43 ± 2.11) were included in the study for further analysis. Thus, a total of 60 restorations were evaluated at 3-month intervals for 18 months (Figure 2). The distribution of the restored teeth is shown in Table 2.
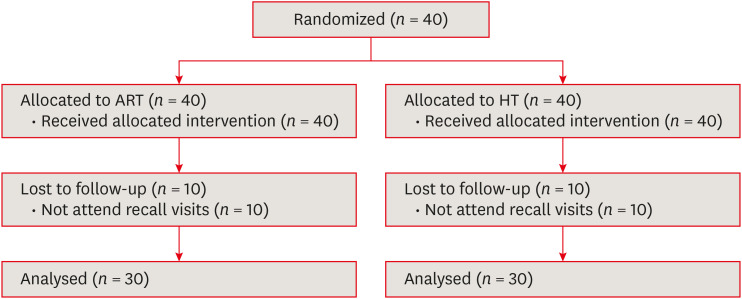
Flow chart of participants.
ART, atraumatic restorative treatment; HT, Hall technique.

The distribution of primary teeth according to techniques
The clinical evaluations of teeth were performed by 2 trained pediatric dentists (C.K. and E.O.). The consistency of operators was measured as ‘almost perfect’ (Cohen’s kappa value = 0.93).
In the clinical evaluations of teeth that were treated with HT, the patients did not have complaints of pain or other symptoms, all crowns remained in the oral cavity, the gums were healthy, and the teeth were functional in all evaluations. The teeth did not respond to percussion and palpation, and there was no plaque accumulation around the crowns. All restorations were scored as “successful,” according to Innes et al.’s outcome criteria for HT treatments [16] (Figures 3 and 4).
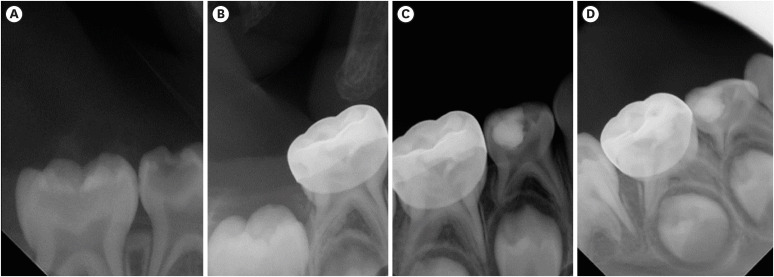
Radiographic images of Hall technique restoration. (A) Before treatment. (B) Six months after treatment. (C) One year after treatment. (D) Eighteen months after treatment.
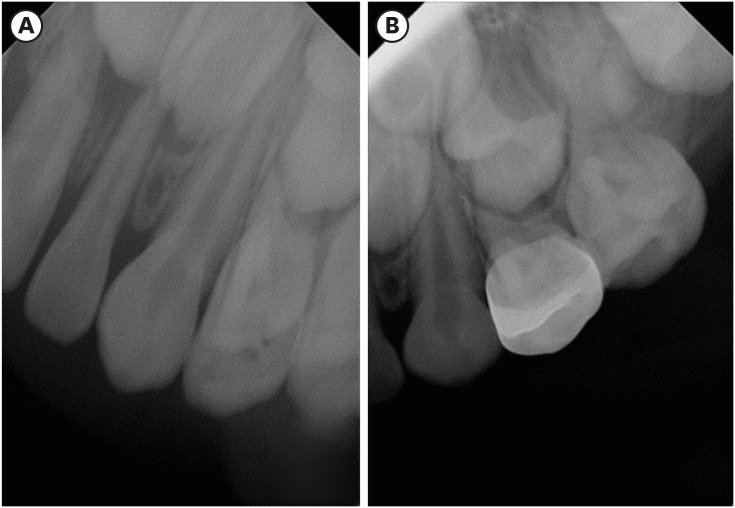
Radiographic images of Hall technique restoration. (A) Before treatment. (B) Baseline treatment.
In the clinical evaluations of ART restorations at 3 and 6 months, all restorations received A scores in all evaluation criteria; however, at the 9-month follow-up evaluations, B scores started to be observed for surface texture and marginal integrity, and the number of restorations that received a B score in these criteria increased after the clinical evaluation 12 months after treatment. At the end of the 18-month follow-up period, according to the surface texture and marginal integrity, the percentages of B score were recorded as 26.7% and 33.3%, respectively. No restoration received a Charlie score, and there was no plaque accumulation in the restored teeth. In comparing the ART restorations at different follow-up intervals using the McNemar test, no statistically significant differences between the rates were found (P > 0.05). The evaluations of restorations according to the surface texture and marginal integrity criteria are shown in Tables 3 and 4.

The number of ART restorations with B and C scores for surface texture according to the months and teeth

The number of ART restorations with B and C scores for marginal integrity according to the months and teeth
In both groups, no pathological conditions were observed in the radiographic evaluations during the follow-up intervals, including external/internal root resorption, radiolucency in the bifurcation region, enlargement of the periodontal ligament space, and ectopic eruption of the permanent first molar tooth adjacent to the placed crown. All restorations were considered successful in terms of radiographic evaluation.
Performing statistical comparisons of the clinical and radiographic evaluations between the HT and ART restorations was not possible due to the 100% success rates of the 2 techniques. The oral hygiene of patients also improved throughout the follow-up periods. When the patients were asked about their satisfaction with the treatments during the 18-month follow-up, the children who underwent HT restorations stated that they did not have any complaints when they did not go to school, but they were not satisfied with the metal appearance of the crown aesthetically after they started to attend school (n = 3). This was not the case for ART, as all patients stated that they were satisfied in terms of aesthetics.
DISCUSSION
In our study, we aimed to evaluate the 18-month outcomes of the 2 techniques by applying HT to one of the cavitated primary molars and ART to the symmetrical molars of children with cooperation problems. We planned to evaluate whether the success of ART, which can be applied in cases in which clinical conditions cannot be provided, is similar to the success of HT, which can be applied under clinical conditions, and to assess the applicability of ART in children who cannot be administered HT. In addition, we attempted to achieve standardization by applying both treatments in the teeth of the same child in whom the caries lesion has progressed to the middle 1/3 of the dentin to ensure the same nutrition, oral hygiene, and saliva environment.
Today, with the prominence of minimally invasive treatments, the application of ART and HT in pediatric patients has come to the fore as an alternative to conventional techniques. Selective removal of caries using the ART technique has been shown to be more advantageous than conventional methods, and these treatments have been shown to be more successful than conventional restorative treatments [10141718]. In this technique, since tertiary dentin formation leads to the inactivation of the carious lesion, the use of GICs in ART has been at the forefront of treatment strategies, and it has recently been reported that HVGICs can be used successfully for treating single-surface carious lesions in primary teeth [19202122]. In our study, ART restorations were performed using HVGIC.
In addition to the studies showing that the HT, in which SSC is placed without caries removal, is more successful than conventional restorative treatments, it has also been stated that there is no significant difference between HT and conventional SSC placement in which occlusal reduction was performed [10142324252627]. In HT treatments, the stimulus causing pain can be eliminated by placing a dressing on teeth presenting with short-term provoked pain and reversible pulpitis, and the pulp tissue can be relieved for reparative dentin formation [10]. Therefore, in our study, although the 18-month results of both techniques were evaluated in anxious children aged 5–6 years, it is thought that similar findings may have been obtained if the patients were assessed for only the first 6 months after treatment.
The results of the present study showed that HT was successful in the treatment of primary molars with occlusal caries, presenting high clinical and radiographic efficacy with no minor or major failures (100% success). In this study, the observation period of primary molars treated with HT was 18 months, while in other studies follow-up ranged from one to 3 years, and high survival rates of HT (92%–98.9%) have been reported [1116232427282930]. The high success rates of the HT can be attributed to the fact that complete isolation of the plaque biofilm from the oral environment slows or stops the progression of the lesion, increasing the durability of the crown and the GIC providing remineralization of the lesion [1731]. In contrast to the success rates of more than 90% reported in studies with similar follow-up periods, the survival rates of the HT restorations after 3 and 5 years were lower (73.4% and 67.6%, respectively) in a retrospective study [4]. When comparing data across studies, it should be noted that factors such as different outcome measures and evaluation criteria for ascribing restoration success or failure, design and setting of the studies, and characteristics of the operators affect the findings.
Regarding factors related to teeth, the type of restoration is a factor associated with the success rate of ART restorations [32]. Single-surface ART restorations have higher survival rates than multiple-surface restorations in primary teeth [2122333435]. The success rate of single surface ART at 1-year follow-up ranged between 95% and 100%, but decreased to 96.7%–91% and 86% at 2- and 3-year follow-ups, respectively [3637]. For multiple-surface cavities, the survival rate according to the criteria evaluated has been shown to be 55% and 65.4% after 1- and 2-year studies, respectively [3334]. Because of the unacceptably high failure rates for ART, this technique is not recommended for multiple-surface restorations in primary teeth [38]. It is thought that differences in the structural properties and preparation methods (hand-mixed or encapsulated) of GICs used in ART restorations may affect the results. A study that assessed the 3-year cumulative survival rate of single-surface ART restorations placed in posterior primary teeth in persons with disability showed the cumulative survival rates for restorations were 100% for ART [21]. Although there are differences between our study and the cited study, such as the age of the participants and the characteristics of the study sample, in line with their findings, the success rate of single-surface ART restorations was 100% during the follow-up period in our study. The higher success rate in this study is due to the single-surface restorations, which made it easier to prevent the contamination of the cavity with saliva and blood compared to restorations with approximal cavities, and improvements in the ART approach, as HVGIC was used. Although it was stated that the coating agent added to the surface of the glass-ionomer system contains a nano-filled resin that may have contributed to the increased resistance of the material to mechanical forces, in multiple-surface cavities, the insufficient flexible strength of HVGICs limits the longevity of the material used in ART restorations [739].
In our study, both techniques used to perform single-surface restorations achieved successful results. It is undisputed that HT will be more successful in multi-surface cavities, as SSC distributes chewing forces over the entire surface. Therefore, when the number of surfaces increases, it is not possible to make a comparison between the restorations with ART and SSC. Increasing the number of studies on this subject will help guide dental professionals in deciding in which cases the techniques should be applied in the clinic. In this study, the clinical and radiographic success of both techniques showed that these techniques can be applied to anxious children. In addition, the ease of application of ART and the completion of treatment in a shorter time are among the advantages of this technique.
In addition to the clinical and radiographic outcomes determined by clinicians, patient-based results from studies evaluating ART and HT have also been reported. Compared to other restorative procedures using rotary instruments, both methods have been reported to cause less anxiety in children and minimize dental fear in preschool children in whom ART restorations are applied, making this method more acceptable than conventional methods [54041]. In a given study population with children of 5 years of age, the ART approach was also well accepted [6]. In our study, when evaluating patient satisfaction, there were no complaints or aesthetic dissatisfaction in children who underwent this technique, even if slight deteriorations occurred in ART restorations. Although HT in primary molars was shown to be well-tolerated by children and acceptable by parents, objections to the appearance of crowns were reported by around 5% of parents [14424344]. Although children were not deceived by appearances and had a positive attitude about crowns, 10% of the school-age children with any complaints were not satisfied with the appearance of crowns and demanded that the crowns be removed in the study [41].
The present study has some limitations. Firstly, the 18-month follow-up period of the study and the loss of participants during the follow-up period may have affected the results and failure rate. Due to the lack of a failure in either group, we could not perform a statistical comparison. Despite the limitations, the findings of this study are important because it is the first study to our knowledge to evaluate success rates of 2 techniques in posterior primary teeth in Turkish primary care. Another strength of this study is that both clinical and radiographic examinations were performed to evaluate the success rates of the 2 techniques.
CONCLUSIONS
The 18-month clinical and radiographic results after treatments applied to single-surface cavities in anxious and fearful children showed that both treatment methods were successful in meeting the demands and needs of the patients. Although HT is also successful, dental professionals should consider applying ART in the treatment of some children for aesthetic reasons.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: Kırzıoglu Z.
Data curation: Kale C.
Formal analysis: Oz E.
Funding acquisition: Kale C.
Investigation: Oz E, Kale C.
Methodology: Kırzıoglu Z.
Project administration: Kırzıoglu Z.
Resources: Kırzıoglu Z, Kale C.
Software: Kırzıoglu Z.
Supervision: Kırzıoglu Z.
Validation: Oz E, Kırzıoglu Z.
Visualization: Oz E.
Writing - original draft: Oz E, Kırzıoglu Z, Kale C.
Writing - review & editing: Oz E, Kırzıoglu Z, Kale C.



