Successful nonsurgical treatment of type II dens invaginatus with 5 root canals using a self-adjusting file: a case report
Article information

Abstract
The present report describes the endodontic treatment of an Oehlers type II dens invaginatus in a maxillary lateral incisor with 5 root canals, an extremely rare condition. Apical periodontitis and related symptoms were noted. Cone-beam computed tomography was used to aid the diagnosis, reveal tooth morphology, and assist in canal location. The pulp chamber was carefully accessed, and the root canals were explored under magnification. All root canals were prepared with an R25 Reciproc Blue system and sodium hypochlorite (NaOCl) irrigation. After initial preparation, a self-adjusting file (SAF) with NaOCl and ethylenediaminetetraacetic acid was used to complement the disinfection. Additionally, calcium hydroxide medication was applied. Vertical compaction was used to fill the canals with a calcium silicate-based endodontic sealer and gutta-percha. After 12 months, the patient exhibited healing of the periapical region, absence of symptoms, and normal dental function. In conclusion, this nonsurgical treatment protocol was successful in promoting the cure of apical periodontitis. Both complementary disinfection with an SAF and use of calcium hydroxide medication should be considered when choosing the best treatment approach for dens invaginatus with very complex anatomy.
INTRODUCTION
The anatomical complexity of the tooth influences the success of endodontic treatment, since access to and disinfection of the root canal system can be difficult [12]. Dens invaginatus is a dental anomaly characterized by the deepening of the enamel organ in the dental papilla during tooth formation, producing substantial variation in the root canal anatomy [3].
Several classifications exist for dens invaginatus, of which the Oehlers classification system is the most popular [4]. According to this system, in type I, enamel invagination is limited to the area of the dental crown, while in type II, invagination extends beyond the cementoenamel junction to the root. In type IIIa, enamel invagination reaches the apical region of the tooth, forming multiple apical foramina. The invagination communicates with the periodontal ligament via a lateral foramen. In type IIIb, the anatomy of the invagination and pulp resembles that of type IIIa; however, the invagination communicates with the periodontal ligament via an apical foramen.
The reported prevalence of dens invaginatus ranges from 0.04% to 10%, and most cases affect the permanent upper lateral incisors [56]. Teeth with dens invaginatus often become infected due to oral communication through the opening of the invagination, requiring endodontic treatment or extraction. Endodontic treatment of a tooth with dens invaginatus is a potentially complicated procedure [7].
To overcome the limitations of current instrumentation techniques, the self-adjusting file (SAF) system was introduced to the market. The SAF system consists of a single-use file manufactured from a nickel and titanium alloy, and it differs from rotary systems particularly in its innovative design, operational mode, and irrigation system. The system was designed to adapt to the cross-sectional shape of the root canal and is used by scraping the dentin with low-amplitude in-and-out movements [8].
Cone-beam computed tomography (CBCT) has been used to map the root canal morphology in a way that allows a 3-dimensional assessment of the external and internal anatomy. This feature is especially relevant to the detailed study of dens invaginatus configuration. In a comparison of CBCT images of extracted teeth with routine 2-dimensional radiographic images of the same specimens, the CBCT images consistently showed greater numbers of identified root canals [9].
In the present study, complementary disinfection strategies with an SAF and calcium hydroxide medication are reported for the nonsurgical endodontic treatment of an Oehlers type II dens invaginatus in a maxillary lateral incisor with 5 root canals.
CASE REPORT
This case report was written in compliance with the Preferred Reporting Items for Case Reports in Endodontics 2020 guidelines [10]. A 12-year-old normosystemic female patient presented to the Dentistry School Clinic of Centro Universitário Christus in Fortaleza, Brazil, reporting a history of edema and fistula in the upper right lateral incisor region. The patient’s previous dental history was noncontributory. A clinical examination revealed a groove in the cingulate region and a sinus tract that was tracked with a gutta-percha cone to the apical area of the referred tooth. An unusual volume of enamel was also observed on the palatal side of the crown (Figure 1). Informed consent was obtained from the patient’s parents for the present report.

Clinical aspect of the tooth crown and initial radiographic image.
A periapical radiograph revealed an area of periapical bone rarefaction and type II dens invaginatus (Figure 1). A medium-volume CBCT scan (iCat CBCT, Imaging Sciences International, Hatfield, PA, USA) was performed at 90 kVp and 4 mA. The imaging area was a 12-cm-high and 12-cm-diameter cylinder with 0.10-mm voxel reconstruction. Dens invaginatus and apical periodontitis were confirmed by CBCT (Figure 2). A pulp sensibility test with a cold stimulus using a cotton pellet and refrigerant gas (EndoFrost, Wilcos, Petrópolis, RJ, Brazil) was negative, but the patient reported pain during the apical palpation and vertical percussion. Asymptomatic apical periodontitis was diagnosed, and endodontic treatment was indicated.
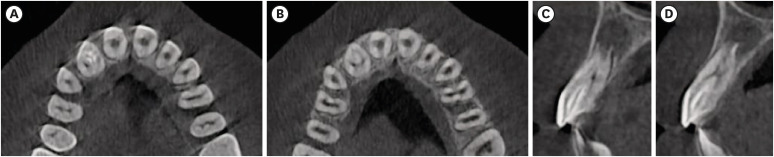
Cone-beam computed tomographic images.
First, anesthesia with 3% mepivacaine without vasoconstrictor (Dentsply Sirona, Charlotte, NC, USA) was applied. This substance was chosen to reduce the post-treatment anesthetic effect and to prevent the patient from biting her lips after the consultation. The patient’s parents had reported this occurring at other times. Next, coronal access was gained through the palatal region. Then, a rubber dam was applied, and initial root canal exploration was performed with a size 10 K-file (Dentsply Maillefer, Ballaigues, Switzerland). With a clinical microscope (Alliance, São Carlos, SP, Brazil), 5 root canals were located, one of which was the pseudo-canal associated with the invagination. The invagination was centrally positioned relative to the true root canals, which surrounded most of the invagination perimeter up to an extent in the root, as demonstrated in the access cavity (Figure 3). The 2 true canals in the mesiopalatal position had separate entrances, as did the 2 distopalatal canals. However, each pair was connected in the middle third of the root. All root canals, including the pseudo-canal, were fully accessed during the exploration from the opening to the apex.
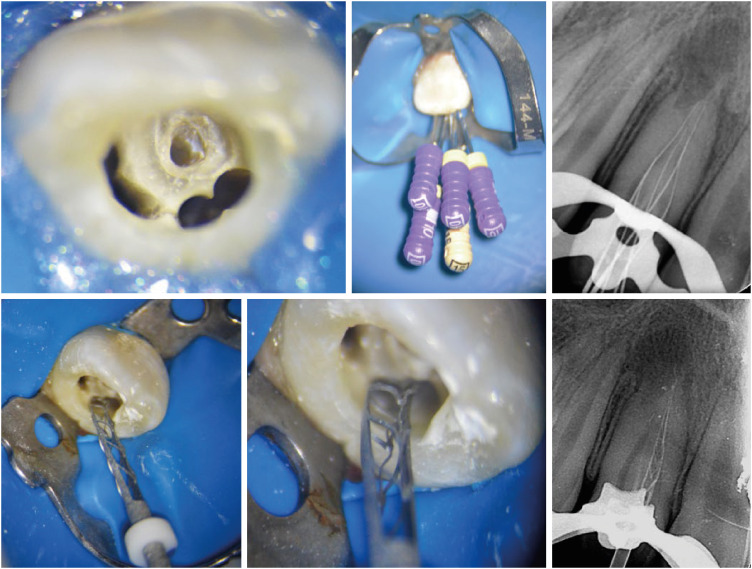
Access cavity including both the true root canal and the invagination and root canal exploration (clinical and radiographic views).
The working lengths were confirmed with an electronic apex locator (from the VDW Gold motor, VDW, Munich, Germany), and root canal preparation was performed with a Reciproc Blue R25 instrument (VDW) for all canals using reciprocating movement (VDW Gold motor, VDW). Abundant irrigation with 2.5% sodium hypochlorite (NaOCl, Biodinâmica, São Paulo, SP, Brazil) was performed during root canal preparation, delivered with a 30-G NaviTip needle (UltraDent, Salt Lake City, UT, USA). Furthermore, each canal was irrigated with 17% ethylenediaminetetraacetic acid (EDTA, Biodinâmica) for 3 minutes to facilitate dentinal debris removal. Afterward, a 1.5-mm SAF system (ReDent Nova, Tel Aviv, Israel) was used to complement the root canal disinfection. The SAF instrument was operated with an in-and-out motion to the working length for 1 minute of activation under continuous irrigation with 2.5% NaOCl (flow rate of 5 mL/min, VATEA, ReDent Nova). This procedure was repeated 2 more times, for a total of 3 cycles. Each pair of true canals (2 mesiobuccal and 2 distobuccal) was united during treatment. The canals were washed with 17% EDTA for 3 minutes and dried with paper points. Intracanal medication containing calcium hydroxide (UltraCal, UltraDent) was inserted into the canals, and a periapical radiograph confirmed adequate filling. The crown was provisionally sealed with glass ionomer cement (Biodinâmica).
After 15 days, the patient reported no symptoms, and the sinus tract disappeared. The intracanal medication was removed with NaOCl and EDTA, and the SAF approach was repeated as described previously. The root canals were dried and filled with gutta-percha and bioceramic sealer (EndoSequence BC Sealer, Brasseler, Savannah, GA, USA) using vertical compaction. Permanent coronal restoration was immediately performed with composite resin (Z250, 3M, São Paulo, SP, Brazil) (Figure 4). After 2 years, the patient remained asymptomatic, and the tooth presented normal aesthetic and masticatory functions. Additionally, the periapical lesion was completely healed, as confirmed radiographically (Figure 5).
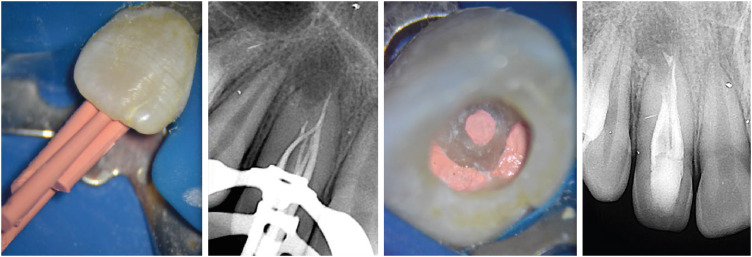
Details of the filling phase.

Clinical and radiographic aspects 2 years after treatment.
DISCUSSION
The number and morphology of root canals in dens invaginatus are highly unpredictable and variable. A rare and very complex root canal morphology, with 5 root canals, was observed in the present case. Using CBCT, Capar et al. [11] studied the prevalence of each Oehlers type of dens invaginatus and concluded that type I was the most common (65.9%), type II was found in only 29.5% of cases, and type III was the least common (4.6%) and the most difficult to treat. Those authors also recommended using CBCT to accurately study the anatomy of the dens invaginatus and determine the best treatment approach.
Several treatment options exist for dens invaginatus, depending on its complexity and the pulp diagnosis. In less complex cases, prophylactic sealing of the invagination and constant monitoring are necessary, as in type I dens invaginatus with vital pulp. Endodontic treatment is necessary if the invagination communicates with the root canal with signs of pulp involvement, as in dens invaginatus types II and III. In rare cases, the invagination does not communicate with the root canal, and the sealing of the invagination and the preservation of pulp vitality can be considered [1213].
The SAF system is highly effective in that it leaves considerably fewer untouched canal areas than conventional rotary or reciprocating systems [1415]. Two main factors justify this difference. First, the SAF is a hollow, flexible file that adapts 3-dimensionally to the root canal shape. This property is beneficial in flat or oval root canals [1516]. Second, the system allows continuous and simultaneous irrigation of the root canal throughout the procedure, with additional activation of the irrigant by its vibrating movement. These aspects facilitate better cleaning of the root canal, especially in areas difficult to access with the irrigant [17]. Given the anatomical complexity of the present case, the SAF was used as a complement to root canal disinfection. A previous study also reported the successful endodontic treatment of an Oehlers type III dens invaginatus using the SAF system in a complementary procedure [12]. The main differences between the studies are that in the prior study, the affected tooth was the maxillary central incisor, and the EndoVac System was used as another complementary step. Additionally, intracanal medication seems to have exerted a decisive role in the present case.
As it remains inside the root canal for a relatively long time, intracanal medication with antibacterial action can reach areas unaffected by instrumentation, contributing to maximum microbial reduction and consequently to the repair of periradicular tissues [181920]. Previous studies corroborate the present findings regarding the use of calcium hydroxide as a complementary disinfecting strategy to treat apical periodontitis of teeth with type II dens invaginatus [212223]. For instance, a recent case series demonstrated the successful treatment of 4 patients with dens invaginatus type II using calcium hydroxide. However, no study has presented 5 root canals, as reported in the present case [21]. Another interesting aspect of these studies is the periapical lesion size, which was relatively large in most cases, including the present study. This fact reinforces the antimicrobial potential of calcium hydroxide, since large lesions usually harbor more microorganisms than small lesions [2425].
CBCT and the operating microscope played a crucial role in the successful management of the aberrant anatomy of the present case. While CBCT helped us better understand the tooth morphology, the surgical microscope enabled more accurate and safe treatment, as demonstrated in previous reports. Nosrat and Schneider [3] reported the success of nonsurgical endodontic treatment of a type IIIb dens invaginatus with 4 root canals using a similar microscope. Agrawal et al. [26] also succeeded in nonsurgical endodontic treatment of a mandibular second premolar with type III dens invaginatus using CBCT for treatment planning.
The strengths and limitations of single reports, such as the present one, should be emphasized. Primary benefits include novelty detection, hypothesis generation, pharmacovigilance, and applicability when other research designs are not feasible. However, the retrospective nature and the inability to establish a cause-and-effect relationship are important limitations. Given these aspects, the present findings cannot be guaranteed in other situations.
CONCLUSIONS
The SAF system and intracanal medication with calcium hydroxide should be considered when choosing the best treatment approach for dens invaginatus with very complex anatomy.
Notes
Funding: This study was supported by grants from Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ) and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq).
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: Candeiro GTM.
Data curation: Menezes AST, Oliveira ACS.
Funding acquisition: Alves FRF.
Writing - original draft: Candeiro GTM, Oliveira ACS.
Writing - review & editing: Alves FRF.