Dentinal tubule penetration of sodium hypochlorite in root canals with and without mechanical preparation and different irrigant activation methods
Article information

Abstract
Objectives
This study evaluated the dentinal penetration depth of 2.5% sodium hypochlorite (NaOCl) in root canals with and without preparation and different irrigant activation protocols.
Materials and Methods
Sixty-three bovine mandibular incisors were randomly allocated to 6 groups (n = 10): G1, preparation + conventional needle irrigation (CNI); G2, preparation + passive ultrasonic irrigation (PUI); G3, preparation + Odous Clean (OC); G4, no preparation + CNI; G5, no preparation + PUI; G6, no preparation + OC; and CG (negative control; n = 3). Samples were filled with crystal violet for 72 hours. Irrigant activation was performed. Samples were sectioned perpendicularly along the long axis, 3 mm and 7 mm from the apex. Images of the root thirds of each block were captured with a stereomicroscope and analyzed with an image analysis software. One-way analysis of variance, followed by the Tukey post hoc test, and the Student’s t-test were used for data analysis, with a significance level of 5%.
Results
The NaOCl penetration depth was similar when preparation was performed, regardless of the method of irrigation activation (p > 0.05). In the groups without preparation, G6 showed greater NaOCl penetration depth (p < 0.05). The groups without preparation had a greater NaOCl penetration depth than those with preparation (p = 0.0019).
Conclusions
The NaOCl penetration depth was similar in groups with root canal preparation. Without root canal preparation, OC allowed deeper NaOCl penetration. The groups without preparation had greater NaOCl penetration than those undergoing root canal preparation.
INTRODUCTION
Regenerative endodontic therapy is defined as a biologically-based procedure designed to replace damaged tooth structures, including dentin and root structures, as well as cells of the pulp–dentin complex [1]. Regenerative endodontic protocols are based on promoting root canal disinfection, inducing the formation of a blood clot in the canal space to serve as a scaffold, and introducing platelet-derived growth factors and mesenchymal stem cells into the canal space to allow tissue formation [23]. Since their introduction as a consistent treatment modality, regenerative endodontic procedures have been used to treat immature permanent teeth with apical periodontitis, promoting greater increases in root length and width and presenting higher survival rates than observed with apexification [345].
In regenerative endodontic procedures, it is recommended not to perform mechanical preparation of the root canal walls in order to avoid possible weakening of the root structure. However, controlling bacterial infection is still the main concern, since the presence of bacteria and their byproducts may negatively affect the formation of dentin-associated mineralized tissue and can jeopardize the success of regenerative procedures [678910]. Therefore, in these situations, disinfection mainly relies on the use of sodium hypochlorite (NaOCl) during irrigation and intracanal medications.
Evidence has been reported regarding the effects of NaOCl on the survival and differentiation of stem cells of apical papilla, the mechanical properties of root dentin, and the expression of growth factors [111213]. Furthermore, it has been well established that activation of NaOCl favors greater dentinal tubule penetration [141516]. However, there is limited evidence regarding NaOCl activation protocols in regenerative procedures. Evidence is available regarding the effects on the mechanical properties of root dentin, the disinfection of large root canals, and on the volumetric extrusion of irrigants, but no studies have investigated NaOCl dentinal penetration depth without root canal preparation [121718].
For these reasons, the aim of this study was to evaluate the dentinal tubule penetration depth of NaOCl when used in root canals with and without instrumentation and using different methods of irrigant activation. The null hypotheses tested were as follow: (i) there would be no differences in the dentinal tubule penetration depth of NaOCl in root canals with and without instrumentation; and (ii) there would be no differences in the dentinal tubule penetration depth of NaOCl in root canals with and without instrumentation regardless of the irrigant activation protocol.
MATERIALS AND METHODS
The research protocol was approved by the Federal University of Rio Grande do Sul’s Ethical Committee for Animal Research (CAEE 204.15919.4.0000.5347).
Sample selection
For this in vitro controlled study, with blinding of the evaluator, sample size calculation was performed using the BioEstat software version 5.0 (Fundação Mamirauá, Belém, PA, Brazil). The following parameters were considered based on a previous study: analysis of variance (ANOVA) and the Tukey test; minimum mean difference between treatments = 3.2%, standard deviation = 1.8, number of treatments = 6, power = 80%, and significance level = 5% [19]. The test calculated a total of 8 samples for each group; however, an additional 20% was considered in case of sample loss. Therefore, 10 samples were planned for the experimental groups, and 3 samples were used as negative controls.
In total, 63 single-rooted freshly extracted bovine incisors were obtained from animals slaughtered for commercial purposes and stored in 0.9% saline solution. Roots with incomplete root formation, fractures, or cracks detected through visual examination and magnification at ×10 were excluded from the study. Bone and gum tissues and the periodontal ligament were removed using Gracey curettes number 3 and 4 (Neumar Instrumentos Cirúrgicos Ltda., São Paulo, SP, Brazil). The crown and coronal aspect of each tooth were removed with a diamond disc, obtaining 11-mm-long roots. Only roots presenting a foraminal diameter equivalent to a size 35 K-file, determined by passively inserting the instrument at the apical constriction, were included.
Experimental groups
Roots were randomly allocated to 6 groups (n = 10), as follows: G1, with root canal preparation + conventional needle irrigation (CNI); G2, with root canal preparation + passive ultrasonic irrigation (PUI); G3, with root canal preparation + Odous Clean (OC); G4, without root canal preparation + CNI; G5, without root canal preparation + PUI; G6, without root canal preparation + OC; GC, negative control (n = 3).
All experimental groups were irrigated with 2.5% NaOCl using a 5-mL syringe (Ultradent Products Inc., South Jordan, UT, USA) with a 27G Endo-Eze needles (Ultradent Products Inc.). NaOCl solution (2.5%) was prepared immediately before use by diluting a 6% stock solution (EMD Chemicals Inc., Darmstadt, Germany) with distilled water.
Experimental procedures
Dental pulp from all teeth was removed with a sterile barbed broach (Dentsply Maillefer, Ballaigues, Switzerland).
In groups G1, G2, and G3, the working length was established at the apical foramen, and preparation was performed with WaveOne Gold Large (#45.05, Dentsply Maillefer) powered by an electric motor (VDW Silver, VDW Company, Munich, Germany) set in the “WaveOne ALL” program. The canals were irrigated with 5 mL of 2.5% NaOCl, 5 mL of 17% ethylenediaminetetraacetic acid (EDTA, Fórmula e Ação, São Paulo, SP, Brazil), and 5 mL of 0.9% saline solution, and then were dried with WaveOne Gold Large paper points (Dentsply Maillefer).
In groups G4, G5, and G6, only irrigation with 5 mL of 0.9% saline solution was performed, and then the canals were dried with #35 sterile absorbent paper points (Dentsply Maillefer).
After the experimental procedures, all canals were filled with crystal violet using a 5 mL syringe with a 27G Endo-Eze needle (Ultradent Products Inc.), and stored at room temperature for 72 hours. The crystal violet was renewed every 12 hours. Then, canals were washed with 20 mL of 0.9% saline solution.
In GC, the root canals were stained, but no mechanical preparation or irrigation was performed.
Irrigant activation protocols
In groups G1 and G4, syringe irrigation was performed as the final step of the irrigation protocol. The canals were irrigated with 6 mL of 2.5% NaOCl and 5 mL of 0.9% saline solution.
In groups G2 and G5, PUI was performed. The root canals were filled with 2.5% NaOCl and an Irrisonic insert (E1, Helse Technology, Santa Rosa de Viterbo, SP, Brazil), positioned 1 mm short of the working length, was activated with an ultrasonic device (Newtron Booster, Satelec Acteon, Merignac Cedex, France) at a frequency of 30 kHz and a power of 10%. Activation was performed for 3 cycles of 20 seconds each, with 2 mL of 2.5% NaOCl replaced after each cycle, resulting in a total activation time of 1 minute and a total of 6 mL of solution used [20]. After PUI, the canals were irrigated with 5 mL of 0.9% saline solution.
In groups G3 and G6, irrigant activation was performed with OC (Odous De Deus Ind Com. Ltda, Belo Horizonte, MG, Brazil). OC is a plastic instrument, with a #30 tip size and .04 taper, and an “aircraft wing”-shaped cross-section. OC was connected to an electric motor (E-connect, MK Life, Porto Alegre, RS, Brazil), positioned up to the working length, and activated with a reciprocating motion (Reciproc ALL – 300 rpm) for 3 cycles of 20 seconds, according to the manufacturer’s instructions. After each cycle, 2 mL of 2.5% NaOCl was placed in the canals. In total, 1 minute of activation was performed, and 6 mL of solution was used. After activation, the canals were irrigated with 5 mL of 0.9% saline solution.
NaOCl penetration
After the various methods of irrigant activation, all samples were sectioned perpendicularly along the long axis, 3 mm and 7 mm short of the apex, with a slow-speed diamond saw (Isomet 1000, Isomet, São Paulo, SP, Brazil), obtaining 3 slices, corresponding to each root third: cervical (C); middle (M); and apical (A). The samples were manually polished with 400-, 600-, and 1,200-grit sandpaper (3M do Brasil, Sumaré, SP, Brazil), respectively. Images of the top surface of the dentin samples were captured with a stereomicroscope (LeicaM80, Leica Microsystems, Wetzlar, Germany). For the purposes of standardization, all images were captured using the same objective at a fixed resolution and optimal focus, saved in .tiff format and uploaded into ImageJ software (National Institutes of Health, Bethesda, MD, USA).
The penetration of the NaOCl into dentin was analyzed, considering the depth of crystal violet stain that was bleached on the cervical, middle, and apical surfaces of each dentin slice. Images of these surfaces were obtained using a stereomicroscope (LeicaM80, Leica Microsystems). The extension of NaOCl penetration into the dentin, in micrometers, was measured in 4 regions (mesial, distal, buccal, and lingual) of each dentin block using ImageJ software (National Institutes of Health) (Figure 1). The mean value of measurements of the 3 surfaces (cervical, middle, and apical) was considered the final value of dentin penetration for each sample.
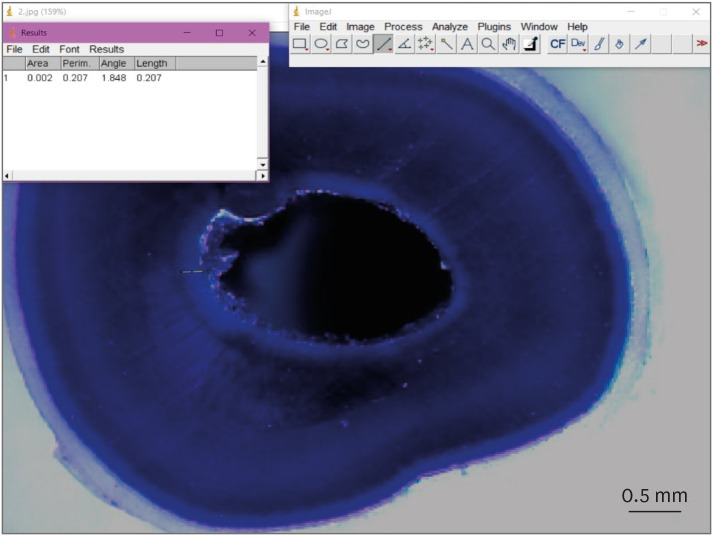
Representative image, using the ImageJ program, showing the measurement of the bleached area promoted by sodium hypochlorite.
Statistical analysis
Data were subjected to statistical analysis using SPSS version 21.0 (IBM Corp., Armonk, NY, USA). The normality of numerical data was assessed using the Shapiro-Wilk test. Intra-examiner agreement was determined by the Cohen kappa coefficient. The Student’s t-test was used to detect statistically significant differences in groups with and without preparation. Intergroup (different methods of irrigant activation) and intragroup (comparison of each third) analyses were performed using 1-way ANOVA and the Tukey post hoc test. The significance level was set at 5%.
RESULTS
Figure 2 presents images of the dentinal penetration of NaOCl in samples from the middle third in groups with root canal preparation (G1, G2, G3, Figure 2A-C); without root canal preparation (G4, G5, G6, Figure 2D-F), and the GC (Figure 2G-I).
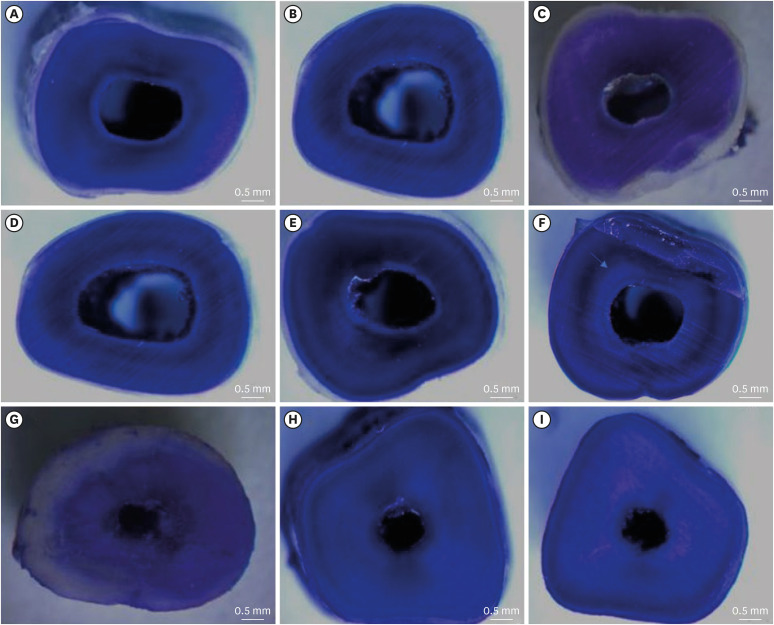
Representative images of the dentinal penetration of sodium hypochlorite in samples from the middle third from groups with root canal preparation (G1-G3: A-C, respectively), without root canal preparation (G4-G6: D-F, respectively), and the GC (G-I).
The level of intra-examiner agreement was substantial, attaining a kappa value of 0.78. The Shapiro-Wilk test indicated a normal distribution of the data.
Table 1 presents data on the dentinal penetration of NaOCl in all experimental groups. In groups without root canal preparation, greater dentinal penetration of NaOCl was observed (p = 0.0019). In groups with root canal preparation, independently of the irrigant activation protocol, the dentinal penetration of NaOCl was similar (p > 0.05). Furthermore, in groups where root canal preparation was not performed, the samples subjected to irrigant activation with OC (G6) showed greater dentinal penetration of NaOCl than the samples that underwent conventional needle irrigation (G4) and PUI (G5) (p < 0.05).

Values of the dentinal penetration of sodium hypochlorite (μm) in groups with and without root canal preparation, after the final irrigation protocols
Table 2 presents data on the dentinal penetration of NaOCl in each root third in all experimental groups. When evaluating the NaOCl penetration into the radicular dentin of each root third, no statistically significant difference was observed in any root third in samples where root canal preparation was performed (p > 0.05). However, in samples where preparation was not performed, G4 (CNI) and G5 (PUI) presented higher NaOCl penetration in the cervical and middle thirds (p < 0.05); while in G6 (OC), a statistically significant difference was observed in the cervical and apical thirds (p < 0.05) (Figure 3).

Values of the dentinal penetration of sodium hypochlorite (μm) in each root third, in groups with and without root canal preparation, after final irrigation protocols
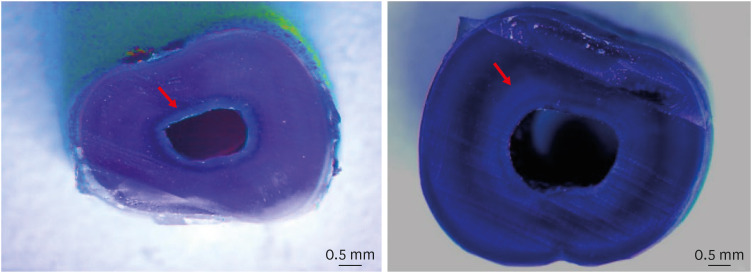
Representative image showing greater penetration of sodium hypochlorite in the cervical third than in the apical third in the G6 group. Arrows indicate the bleached areas.
DISCUSSION
Bacteria can penetrate deeply inside the dentinal tubules and, in immature teeth, bacteria can penetrate even deeper, probably due to the larger diameter of the dentinal tubules in younger patients [21222324]. In regenerative endodontic procedures, reduction of the intracanal microbial load is mandatory in order to achieve success and to allow the formation of dentin-associated mineralized tissue [8910]. However, the American Association of Endodontics and the European Society of Endodontology recommend not performing mechanical preparation of the root canal to avoid possible weakening of the root structure, which could decrease the tooth fracture resistance [67]. Thus, in these situations, disinfection mainly relies on the use of NaOCl and intracanal medications. For these reasons, the present study aimed to evaluate the dentinal penetration depth of NaOCl in root canals with and without mechanical preparation, after different methods of irrigant activation.
In this study, bovine incisors were selected due to the possibility of obtaining fresh and similar samples, allowing standardization of the experimental groups [25]. Furthermore, bovine and human dentin have few differences in the number and diameter of dentinal tubules and dentin permeability, allowing the results to be extrapolated [262728].
Several methodologies have been proposed to evaluate NaOCl penetration into root dentin. Some studies have used fluorescent solutions for subsequent evaluation under a light microscope [14]. Other studies have tested the addition of fluorescent dyes to irrigants for subsequent confocal laser scanning microscopy analysis [2930]. These methodologies were not used in the present study because the oxidizing nature of NaOCl may impact the fluorescent ability of the dye and the solutions may not present the same capacity to penetrate into the dentinal tubules as the tested irrigants [13]. Therefore, in this study, NaOCl penetration was evaluated by staining the samples with crystal violet, as previously proposed [31]. This methodology is based on the oxidizing effect of NaOCl, which bleaches the crystal violet. As NaOCl must penetrate into the dentin to discolor it, the bleached area can be correlated to the NaOCl penetration depth [2131]. Based on the findings of this study, the first null hypothesis was rejected.
In groups where root canal preparation was performed, lower NaOCl penetration was observed than in groups without instrumentation, regardless of the method of irrigant activation. This result is probably related to the deposition of debris inside the dentinal tubules during root canal preparation [32]. Even though EDTA was used, it has been reported that EDTA only decalcified dentin to a depth of 20–30 μm after a period of 5 minutes, while packing of debris can be present inside the dentinal tubules to a depth of 40 μm [32]. These findings lead to the conclusion that the deposition of debris inside the dentinal tubules could compromise the disinfectant ability of NaOCl by inhibiting the irrigant penetration into the dentinal tubules, thereby favoring the maintenance of bacteria inside the tubules.
Furthermore, the removal of the smear layer in the apical third is unpredictable when compared to the cervical and middle thirds, possibly due to the smaller diameter of the dentinal tubules and root canal, which reduces the contact of the irrigant with the dentinal walls and its ability to penetrate the dentinal tubules [33].
Regarding the different methods of irrigant activation tested, the results of this study allow us to reject the second null hypothesis. In groups where no root canal preparation was performed, the overall penetration of NaOCl was higher when activated with OC. A previous study that tested a similar device (Easy Clean, Easy Equipamentos Odontológicos, Belo Horizonte, MG, Brazil) has shown that these instruments can promote greater smear layer removal in the apical third than PUI, probably because they can operate up to the total working length, allowing greater NaOCl penetration into the dentinal tubules in the apical third [34].
The PUI and CNI groups only presented significant differences in the cervical and middle thirds, and although PUI presented greater penetration depth than CNI, the difference was not significant. This can probably be explained by the vapor lock phenomenon, which hampers the irrigant flow in the apical third and decreases the irrigation efficacy, as presented in previous studies comparing PUI and CNI [3536].
Disinfection in regenerative procedures relies on the use of chemical substances, and this study verified that in situations where no mechanical debridement is performed, greater dentinal tubule penetration of NaOCl occurs. However, this study has some limitations. It is not possible to infer that this improved dentinal penetration of NaOCl will favor a greater disinfection capacity under clinical conditions. In addition to the effects on biofilm, NaOCl reacts with pulp tissue and dentin inorganic and organic compounds, decreasing the available chlorine and antimicrobial activity [37]. Thus, although it is well established that an increased contact time and volume of NaOCl are factors that influence biofilm removal, further studies are necessary to confirm the hypothesis that greater dentinal penetration, in situations where no mechanical preparation is performed, could favor more extensive disinfection [15].
Finally, 2 protocols were tested prior to crystal violet staining. In G1–G3, root canal preparation was performed by using 2.5% NaOCl and 17% EDTA as chemical substances, while in G4–G6 the canals were only irrigated with 0.9% saline solution. It is known that the use of NaOCl and EDTA can promote alterations of the collagen ultrastructure and erosion of peritubular and intertubular dentin [38]. This may have impacted the penetration capacity of the crystal violet dye, but this possibility could not be measured in the present study. However, it is important to emphasize that in a clinical situation, root canal preparation is performed by means of mechanical debridement associated with chemical solutions, mainly NaOCl and EDTA. Thus, the use of saline solution during root canal preparation does not reflect the clinical situation, meaning that the present results cannot be directly extrapolated.
CONCLUSIONS
Based on the findings of this study, NaOCl penetration into the dentinal tubules was similar in groups where root canal preparation was performed, regardless of the methods of irrigant activation tested. When root canal preparation was not performed, NaOCl showed improved dentinal tubule penetration, with OC promoting deeper penetration.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization:de Oliveira RA, Só MVR.
Data curation: de Oliveira RA, da Rosa RA, Souza MA, Só MVR.
Formal analysis: de Oliveira RA, da Rosa RA, Só MVR.
Investigation: de Oliveira RA.
Methodology: Só MVR.
Project administration: Só MVR.
Supervision: da Rosa RA, Só MVR.
Writing - original draft: de Oliveira RA, da Rosa RA, Só MVR.
Writing - review & editing: Weissheimer T, Só GB, Souza MA, Ribeiro RG.

