Proximity of maxillary molar apexes to the cortical bone surface and the maxillary sinus
Article information

Abstract
Objectives
This study aimed to analyze the proximity of maxillary molar roots to their overlying cortical bone surfaces and the maxillary sinus.
Materials and Methods
Cone-beam computed tomographic images of 151 patients with completely erupted upper molars that had 3 separate roots were studied. The following distances were measured: from the root apex to the cortical plate and maxillary sinus floor, and from the apical 3-mm level of the root to the cortical plate. Differences between groups were analyzed with 1-way analysis of variance and the Scheffé post hoc test, the significance of differences between cone-beam computed tomography views with the paired t-test, and the significance of differences among age groups with linear regression analysis. The significance level was set at p < 0.05.
Results
The mesiobuccal and distobuccal root apexes of maxillary second molars were more distant from the buccal cortical plate than the maxillary first molars (p < 0.05). The apical 3-mm level of the mesiobuccal root of the first molar was closer to the buccal cortical bone than the second molar (p < 0.05). In the maxillary first molars, the thickness of the buccal cortical bone decreased in all roots with age (p < 0.05). In all root apexes of both molars, the difference in the vertical level between the maxillary sinus floor and the root apex increased with age (p < 0.05).
Conclusions
Awareness of the anatomical profile of maxillary molar apices in relation to the cortical bones and maxillary sinus will be beneficial for apical surgery.
INTRODUCTION
In planning apical surgery for molar teeth, the surgeon must be sure of the exact apex location and must determine the proximity of the neighboring anatomic structures, including the cortical bone and maxillary sinus [123]. From a surgical standpoint, it is most challenging to precisely ascertain where the apex is located in the molar region. To expose the root apices accurately, osteotomy (i.e., removal of the cortical plate) must be performed carefully after locating the apex on radiographs [1].
Unlike the mandibular molar roots, the maxillary molar roots are located near the maxillary sinus [4]. Due to their close location, periapical lesions originating from the maxillary molars can influence the maxillary sinus, and apical surgery on the maxillary molars may harm the sinus. Several studies have reported maxillary sinus infections transmitted from the maxillary molars [56789]. Watzek et al. [10] showed that 28% of endodontic surgical cases resulted in maxillary sinus perforations. These reports indicate the importance of understanding the anatomical relationship between the molar roots and their adjacent structures for maxillary molar surgery.
Computed tomographic (CT) scans have made it possible to evaluate bony lesions and their relationship to adjacent anatomical structures [11]. Furthermore, CT scans may provide information regarding the lesion and the healing pattern of bone after endodontic treatment [1213].
The recently developed modality of cone-beam computed tomography (CBCT) has significant advantages over traditional periapical or panoramic radiographs, especially for the localization and evaluation of periapical or periodontal lesions. A systematic review found that CBCT was more effective than conventional radiography for visualizing the location of impacted teeth [14]. Another study compared conventional radiographs and CBCT for periapical and maxillary sinus evaluations and reported that CBCT was significantly more accurate than conventional imaging for identifying lesions and their proximity to the maxillary sinus [15].
Because CBCT scans provide 3-dimensional information on anatomic structures and allow the recognition of the spatial relationship of roots with adjacent structures, the cortical bone thickness over the molar roots and their proximity to the maxillary sinus can be ascertained with CBCT when planning an endodontic surgical procedure for the upper molars.
Therefore, this study aimed to analyze the proximity of the maxillary molar roots to their overlying cortical bones and the relationship between the maxillary molar root and the maxillary sinus by using CBCT images.
MATERIALS AND METHODS
This study received approval from the Institutional Review Board (KNUDH-2020-04-04-01). The PRIRATE 2020 flowchart for the research is shown in Figure 1. Imaging records were retrieved from the archives of the Kyungpook National University Dental Hospital in 2019 and 2020. The scanned data were from the Korean population. CBCT scans were obtained using a Pax-Flex 3D imaging system (Vatech, Seoul, Korea) operating at 5 mA and 89 kV, with a 24-second scanning time. Data containing small-volume CBCT scans were evaluated. The CT images were taken with 0.2-mm-thick cross-sectional slices in a 12 × 12 × 8.5 cm field of view using a high-resolution bone algorithm. The reconstruction matrix was 416 × 416 pixels. The images were reconstructed and saved using Ez3Dplus software (Vatech America Inc., Fort Lee, NJ, USA) and a picture archiving and communication system (PACS). The inclusion criteria were as follows: patients at least 17 years of age who had maxillary molars with 3 separate roots. The exclusion criteria were cases missing at least 1 of the 4 maxillary molars, with an apical lesion close to the cortical bone or maxillary sinus, and with teeth that had only 1 or 2 roots. In total, 151 cases (91 men and 60 women) were selected for this study. This study included 298 maxillary first molars and 269 maxillary second molars from patients with a mean age of 33 years (ranging, 17–81 years) (Table 1).
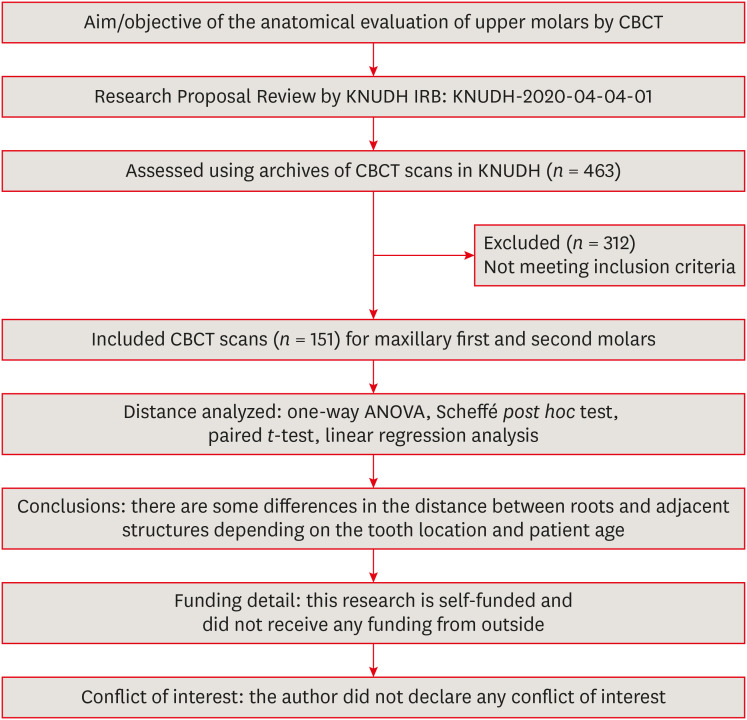
PRIRATE 2020 flowchart for the experimental design.
CBCT, cone-beam computed tomography; KNUDH, Kyungpook National University Dental Hospital; IRB, Institutional Review Board; ANOVA, analysis of variance.

Data on the cases included in this study
Data acquisition
All teeth were analyzed by measuring the distance from the adjacent buccal or palatal cortical plate to the root apex and to the center of root at 3.0 mm from the apex (Figure 2), and the difference in the vertical level from the sinus floor to the root apex. The vertical relationship between the maxillary molar apex and maxillary sinus was categorized as follows (Figure 3): type I, protrusion of the root apex into the sinus; type II, the root apex at the same vertical level as the sinus floor; and type III, location of the root apex below the sinus floor.
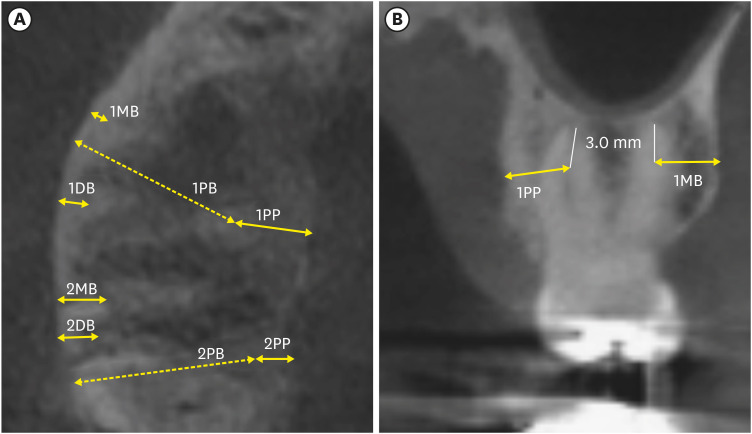
Measurements of root distance from the cortical bone. A. Measurements of the maxillary molar root apex from the axial view of cone-beam computed tomography (CBCT). B. Measurements at the apical 3-mm level of the root from the coronal view of CBCT.
1MB, distance between the first molar mesiobuccal root and the buccal cortical plate; 1DB, distance between the first molar distobuccal root and the buccal cortical plate; 1PB, distance between the first molar palatal root and the buccal cortical plate; 1PP, distance between the first molar palatal root and the palatal cortical plate; 2MB, distance between the second molar mesiobuccal root and the buccal cortical plate; 2DB, distance between the second molar distobuccal root and the buccal cortical plate; 2PB, distance between the second molar palatal root and the buccal cortical plate; 2PP, distance between the second molar palatal root and the palatal cortical plate.
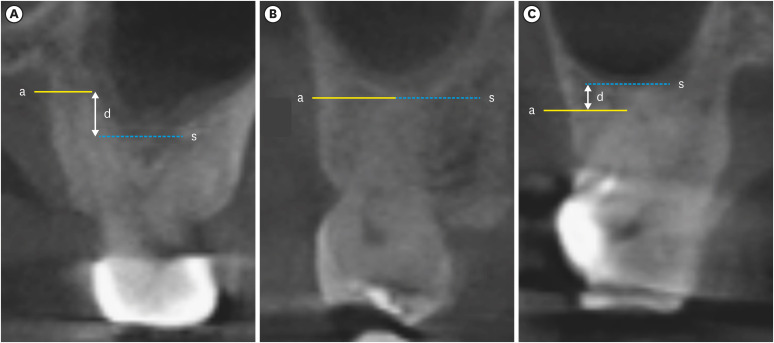
The vertical relationship between the maxillary molar apex and the maxillary sinus floor. (A) Type I, the root apex protruded into the sinus; (B) type II, the root apex was 0 mm from the sinus floor or was at the same vertical level as the sinus floor; and (C) type III, the root apex was below the sinus floor.
a, level of root apex; s, level of maxillary sinus floor; d, level distance between root apex and sinus floor.
On the axial and coronal views of the CBCT scans, the distance was measured (Infinitt PACS, Infinitt, Seoul, Korea) in millimeters. The measured values were grouped according to the tooth location and the age of the patient.
Statistical analysis
Means ± standard deviations (SD) were calculated. To evaluate the differences between groups, 1-way analysis of variance and the Scheffé post hoc test were used. The paired t-test was used to test the significance of differences between CBCT views. Linear regression analysis was used to test the significance of differences among age groups. A p value < 0.05 was considered significant. All statistical analyses were performed with SPSS version 21.0 (IBM Corp., Armonk, NY, USA).
RESULTS
The distance between the root apex and the cortical bone
In both axial and coronal views, the mesiobuccal and distobuccal root apexes of maxillary second molars showed greater distances from buccal cortical bone than the maxillary first molars (p < 0.05).
Among the buccal root apexes of the maxillary molars, the closest root to the buccal cortical bone plate was the first molar’s mesiobuccal root apex (average value: 3.34 mm) as measured in the axial view (Table 2). The mesiobuccal root of the second molar showed the thickest buccal cortical bone among the buccal roots (average value: 5.56 mm). The average distance between the palatal root apex and the palatal cortical bone was 3.52 mm and 3.24 mm in the first and second molars, respectively.

The distance from 3-rooted maxillary molar root apexes to the adjacent cortical bone in the axial view (mm)
The distance between the 3-mm level from the root apex and the cortical plate
The mesiobuccal root of the first molar was closer to the buccal cortical bone than the same root of the second molar (p < 0.05).
In the coronal plane, the closest point to the cortical bone was between the palatal root of the first molar and the palatal cortical plate (average: 3.73 mm) (Table 3). The mesiobuccal root of the second molar showed the thickest buccal bone among the buccal roots (6.01 mm).

The distance from the 3-mm level from the root apex to the adjacent cortical bone in the coronal view (mm)
The proximity of the root apex to the overlying cortical bone in relation to age
A comparison across different age groups is shown in Table 4. In the maxillary first molar, the buccal bone thickness tended to decrease in all roots with age (p < 0.05), and in the second molar had thinner buccal cortical bone with age (linear regression analysis, p < 0.05).

The distance from the root apex to the buccal cortical bone in relation to age in the axial view (mm)
The vertical relationship and distance from the root apex to the maxillary sinus floor
Cases where the root apex protruded into the maxillary sinus were marked as negative values (Tables 5 and 6). The mesiobuccal root apex of the second molars showed more frequent type I and less frequent type III configurations than those of the first molars. The mesiobuccal root apex of the second molars was closer to the maxillary sinus floor than that of the first molars, albeit without statistical significance. Only the mesiobuccal root apex of the maxillary second molar slightly protruded into the maxillary sinus (average: 0.1 mm). The palatal root apex of the second molars was located further from the maxillary sinus floor than that of the first molars (p < 0.05).

The vertical relationship between maxillary molar apexes and the maxillary sinus (coronal view)

The distance from the root apex to the maxillary sinus floor according to age (mm)
In all root apexes of both molars, the vertical distance between the maxillary sinus and the root apex increased with age (linear regression analysis, p < 0.05) (Table 6).
DISCUSSION
The present study used CBCT scans to analyze the proximity of the root apex of maxillary molar teeth to cortical bone and the maxillary sinus. Through endodontic microsurgery, the cause of failure of previous non-surgical root canal therapy can be effectively removed, including remaining pathogens in the apical area [1617]. When planning apical surgery, it is necessary to accurately evaluate the surrounding structures because the surgical procedure includes osteotomy and root resection. Therefore, the spatial relationship between the root apex, overlying cortical bone, and the maxillary sinus is a very important factor [18].
In the present study, root apexes were used as anatomical landmarks, the proximity of which to the cortical plate and maxillary sinus was analyzed. Even though a single mesiobuccal root may contain 1, 2, or 3 canals and an isthmus in between, 1 prominent root apex of the mesiobuccal root was used as an anatomical landmark [19].
In this study, the mesiobuccal and distobuccal root apexes of maxillary second molars were more distant from the buccal cortical bone than those of maxillary first molars. This finding for the maxillary molars is in accordance with the previous finding for the mandibular molars, in that the buccal cortical bone is thicker in the second molar than in the first molar [20]. In previous studies, the mesiobuccal root of the upper second molar was located farthest from the buccal cortical plate. However, this root was the closest to the maxillary sinus floor [212223].
In the present study, there was a tendency for buccal cortical bone thickness to decrease with age, especially over the maxillary first molar roots. This finding may be related to factors such as vitamin D deficiency, decreased osteoblast function, decreased growth hormone, and decreased maximum bone mass [2425]. Furthermore, these results also align with a study reporting that skeletal aging starts after an individual reaches peak bone mass, followed by progressive bone loss [26]. That study also showed that changes in bone quality and quantity take place during growth and subsequent aging [26]. A National Institutes of Health report showed that up to 90% of peak bone mass is acquired by age 18 in girls and by age 20 in boys [27].
Some studies have also been conducted on differences in the thickness of buccal cortical bone [172628]. Most of these studies investigated the proximity of the root apex to the cortical plate, but in endodontic microsurgery, the operation is actually performed at the apical 3-mm level. Therefore, in this study, the distance from the apical 3 mm of the root to the cortical bone was also measured. Most irregularities in the root system are located within 3 mm of the apex, and most problems can be eliminated through 3-mm root resection and 3-mm retrograde filling [171829303132]. In the present study, the thickness of overlying cortical bone over the maxillary second molars was significantly greater than that over the first molars, especially on the mesiobuccal root. Therefore, more cortical bone needs to be removed to reach the root of the maxillary second molar than to reach the root of the first molar during surgery.
The maxillary sinus gradually changes in size with age [33]. At the age of 12, it is located at the level of the nasal floor, and at the age of about 20, it reaches its largest size and descends to the lowest point [3435]. Although the relationship between the root of the maxillary molars is affected by changes in the position of the maxilla, little information in the literature exists on whether the position of the teeth in the maxillary molars changes. According to previous studies in Brazil and Turkey, 10% to 14.3% of molar apexes protruded into the maxillary sinus and more than 20% were in contact [3637]. However, a higher percentage of cases showed protrusion into the maxillary sinus in the present study in the Korean population.
In all root apexes of both molars, the vertical distance between the maxillary sinus and the root apex increased with age. This finding may be related to a previous study showing that older patients had smaller maxillary sinuses in terms of volume, regardless of sex and edentulism status [26]. This finding may also be related to another study that found that maxillary sinuses tended to grow smaller with older age [28].
CBCT has recently been used in endodontics increasingly often [38]. CBCT scans provide clinically necessary information that cannot be seen on periapical radiographs [394041]. If the CBCT is performed according to appropriate indications, CBCT may increase accuracy in both non-surgical and surgical endodontics without violating the radiation safety guidelines [42].
CONCLUSIONS
Within the limits of this study, these findings regarding the distance from the maxillary molar root apex to the cortical bone and the vertical relationship of the root apex to the maxillary sinus may provide essential information for clinical endodontic surgery. Understanding the anatomical profile of the maxillary molars in relation to the surrounding cortical bone and maxillary sinus will be beneficial for apical surgery.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: Kim SK, Kim DK, Lee HS.
Data curation: Lee HS.
Formal analysis: Lee HS, Kim SK.
Investigation: Lee HS, Methodology.
Project administration: Kim SK.
Resources: Kim DK, Kim SK.
Software: Lee HS.
Supervision: Kim SK.
Validation: Lee HS, Kim DK, Kim SK.
Visualization: Lee HS.
Writing - original draft: Lee HS.
Writing - review & editing: Kim SK.





