Association between cigarette smoking and the prevalence of post-endodontic periapical pathology: a systematic review and meta-analysis
Article information

Abstract
Objectives
This systematic review and meta-analysis aimed to assess the association of cigarette smoking with the prevalence of post-endodontic apical periodontitis in humans.
Materials and Methods
We searched through PubMed/Medline, Web of Science, and Scopus from inception to December 2020. Risk of bias was performed by using the Newcastle-Ottawa Scale for cross-sectional, cohort, and case-control studies. We performed the statistical analysis in Review Manager 5.3 (RevMan 5.3).
Results
6 studies met the inclusion criteria for qualitative and quantitative synthesis. Statistical analysis of these studies suggests that there were no differences in the prevalence of post endodontic apical periodontitis (AP) when comparing non-smokers vs smoker subjects regarding patients (odds ratio [OR], 0.68; 95% confidence interval [CI], 0.31–1.49; I2 = 58%) and teeth (OR, 1.71; 95% CI, 0.99–2.93; I2 = 72%).
Conclusions
Our findings suggest that there was no association between cigarette smoking and post-endodontic apical periodontitis, as we did not find statistical differences in the prevalence of post-endodontic AP when comparing non-smokers vs smoker subjects. Therefore, smoking should not be considered a risk factor associated with endodontic failure.
INTRODUCTION
Around 16 million people in the world experience serious health problems related to the habit of cigarette smoking (CS). CS causes approximately 7 million global deaths annually, and it is expected that by 2030 tobacco consumption will cause mortality of 10 million people per year [12]. Smokers are more likely to develop cerebrovascular diseases, chronic obstructive pulmonary disease, bronchitis, pneumonia, tachycardia, arterial hypertension, and type 2 diabetes mellitus, as well as neurological degenerations such as depression and cognitive impairment [3]. Furthermore, CS is known to cause deleterious effects on the immune system. Impaired immune reactions related to phagocytosis, neutrophil diapedesis and chemotaxis, in addition to high systemic concentrations of free radical and pro-inflammatory cytokines are directly linked to the release of chemical compounds during tobacco combustion, including nicotine, carbon monoxide, nitrosamine, oxidation radicals, and hydrogen cyanide among others [4567].
Likewise, CS has deleterious effects on local and systemic blood flow, as it causes vascular dysfunction given the modification of the osmotic pressure. Moreover, some chemical compounds of cigarettes such as nicotine induce vasoconstriction, thus restricting the supply of nutrients to tissues and preventing cell proliferation and tissue repair, consequently leading to a progressive tissue breakdown [8910]. Notably, both the immune and vascular systems are key components of all tissue remodeling and healing processes [9].
Endodontic disease manifests both, at pulpal and periapical levels. Pulp and periapical reactions to noxious stimuli are characterized by an initial neurogenic inflammatory response, as the nervous system governs the vascular system by the release of potent vasoactive neuropeptides which act directly on the endothelial and smooth muscle cells, thus affecting the vascular permeability, and exerting pro-inflammatory and immune reactions at the site of the injury [11]. Such inflammatory responses depend on the course, the nature and magnitude of the causal agent, and the ability of the tissue to respond and recover from the noxious stimuli [12].
Several authors have suggested that once the bacterial infection reaches the periapical tissues, smokers are less likely to limit and repair the periapical osteolytic lesion due to the elevated expression of inflammatory mediators, such as tumor necrosis factor-alpha (TNF-α), interleukin 6 (IL-6), C-reactive protein and other substances associated to bone destruction such as reactive oxygen species, collagenase, and serine proteases in addition to elevated levels of carboxyhemoglobin in the blood, which in turn decreases tissue oxygenation and compromise the tissue healing capability in comparison to non-smokers [1213141516]. CS has also been associated with endothelial cell injury and impaired microvascular function [14]. Furthermore, 2 recent systematic reviews evaluated the prevalence of periapical lesions of endodontic origin in endodontically untreated teeth in non-smokers vs smoker patients. These studies concluded that smoker patients are more likely to present apical periodontitis (AP) than non-smokers [1718]. However, much is still not known about the impact of CS on the post-endodontic healing capacity of periapical tissues. Therefore, this systematic review aimed to assess the association of CS with the prevalence of post-endodontic AP in humans.
MATERIALS AND METHODS
A detailed protocol was developed and registered in PROSPERO (CRD42021252542)
This systematic review of the literature was developed following the recommendations of the Cochrane Collaboration and following the PRISMA statement [19].
PICO question
Using the PICO strategy, the focused question and the inclusion criteria were framed:
Population: CS patients.
Intervention: History of conventional root canal treatment (RCT).
Comparison: Non-CS patients.
Outcome: Prevalence of post-endodontic apical periodontitis.
Focused question
In CS patients with a history of conventional RCT, what is the effect of CS on the prevalence of post endodontic AP in comparison with non-smoker patients?
Inclusion criteria
The inclusion criteria were observational studies, reporting the association between CS with the prevalence of post-endodontic AP in smokers vs non-smoker patients. Studies that did not define the evaluation method, in vitro or animal studies, narrative reviews, case reports, and expert opinions were excluded.
Information sources
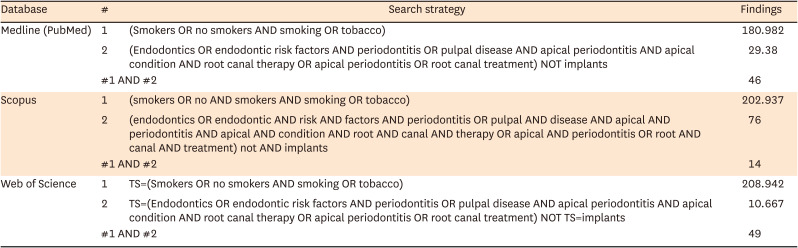
The literature search was conducted following the recommendations of the Cochrane Collaboration. Medical subject headings (MeSH), Emtree language, Descriptors in health sciences (DeCS), and text words related to a complete search strategy were used. Medline (PubMed), Web of Science, and Scopus were searched from inception to December 2020. The search strategy was translated for each database, several keywords were used for each one of the elements of interest and we used the following keyword combinations: 1 AND 2 to report the final results from each database (Appendix 1):
Medline (PubMed) using MeSH terms:
1. (Smokers OR no smokers AND smoking OR tobacco)
2. (Endodontics OR endodontic risk factors AND periodontitis OR pulpal disease AND apical periodontitis AND apical condition AND root canal therapy OR apical periodontitis OR root canal treatment) NOT implants
Scopus using Key word plus:
1. (smokers OR no AND smokers AND smoking OR tobacco)
2. (endodontics OR endodontic AND risk AND factors AND periodontitis OR pulpal AND disease AND apical AND periodontitis AND apical AND condition AND root AND canal AND therapy OR apical AND periodontitis OR root AND canal AND treatment) not AND implants
Web of Science using Key words:
1. TS=(Smokers OR no smokers AND smoking OR tobacco)
2. TS=(Endodontics OR endodontic risk factors AND periodontitis OR pulpal disease AND apical periodontitis AND apical condition AND root canal therapy OR apical periodontitis
To ensure literature saturation, references from relevant articles identified through the search, conferences, thesis databases, Open Grey, Google Scholar, and ClinicalTrials.gov were scanned, among others. There was no language limitation.
Data collection
Two researchers (HM, NR) initially reviewed the titles and abstracts. Then they reviewed the full texts to apply the pre-specified inclusion and exclusion criteria. Disagreements were resolved by consensus and where disagreement could not be solved, a third reviewer decided. Relevant data were collected in duplicate by using a standardized data extraction sheet that contained the following information: author names, year of publication, title, study design, geographic location, objectives, inclusion and exclusion criteria, number of patients included, losses to follow- up, timing, the definition of outcomes, outcomes, association measures, and funding source.
Risk of bias
The assessment of the risk of bias was performed independently by 2 evaluators (OJ, NR) by using the Newcastle-Ottawa Scale for cross-sectional, cohort, and case-control studies [20].
Data analysis and synthesis of results
We performed the statistical analysis in Review Manager 5.3 (RevMan 5.3). We reported the information about categorical variables on odds ratio (OR) with 95% confidence intervals (Cis). We also pooled the information with a random effect meta-analysis according to the heterogeneity expected. Heterogeneity was evaluated using the I2 test. For the interpretation, values of < 50%, and >50% correspond to low, and high levels of heterogeneity, respectively.
Publication bias
There was not enough data to perform this analysis.
Sensitivity analysis
We performed sensitivity analysis extracting weighted studies and running the estimated effect to find differences.
Subgroup analysis
We did not perform a subgroup analysis since we did not have enough data.
RESULTS
Study selection
We initially identified 111 references with the search strategy. After the removal of 14 duplicates, we screened 97 titles/abstracts. Finally, 6 studies met the inclusion criteria for qualitative and quantitative synthesis (Figure 1).
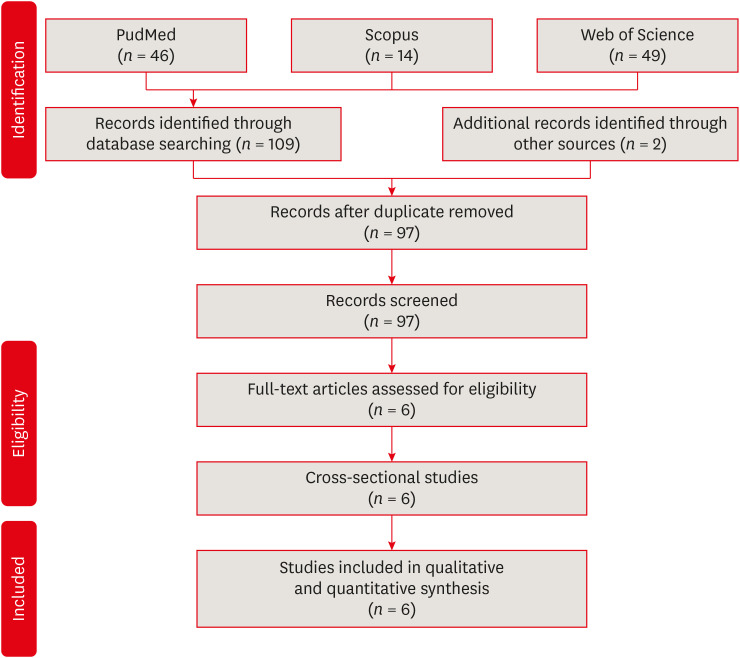
Flowchart of included studies.
Characteristics of included studies
All 6 studies were cross-sectional, published from 2004 to 2020 [212223242526]. The studies compared the post endodontic prevalence of AP in smokers vs non-smokers. The studies were conducted in Croatia, Saudi Arabia, Spain, and Poland. The average group of participants in the studies included individuals between 18 and 65 years. Analysis of these 6 studies shows that the prevalence of post endodontic AP is similar between smokers and non-smokers subjects (Table 1).

Characteristics of studies assessing the post endodontic prevalence of AP in smokers vs non-smokers patient
Risk of bias assessment
Most of the studies had a high risk of bias (66.6%) because they obtained less than 7 points out of 10 possible in the global rating [21222426].
From the evaluation by categories, it can be observed that all the studies included in this systematic review and meta-analysis presented a high risk of bias in the item “selection” since the 6 studies obtained 2 or fewer points out of 5 possible, mainly due to the fact that none of the studies adequately reported on how the calculation to determine the sample size was performed. Furthermore, the determination of the exposure of the subjects to the risk factor was not standardized. On the other hand, only 2 studies used a representative sample of the population through random sampling [2425]; and only 2 studies reported on the characteristics of the excluded or not studied subjects [2325].
In contrast, in the item “comparability “, most of the included studies were evaluated as having a low risk of bias, because they obtained 2 points out of 2 possible [2122232526]. The study performed by Bahammam [24] did not obtain any points in this category, as it did not provide information on how the confounding factors were controlled. Finally, for the item “Outcome/Exposure “all studies [212223242526], were rated as low risk of bias, since they obtained 2 or more points out of 3 possible for this category, mainly because they used objective validated evaluation methods and because they clearly described the statistical tests they used to analyze the data and the level of probability (p-value) (Table 2).

Evaluation according to the Newcastle-Ottawa quality assessment scale
Association between smoking and apical periodontitis.
Regarding the information for patients, we included 3 studies [212425] and found an OR of 0.68 95%CI (0.31 to 1.49) I2: 58%. There were no differences between smokers and no smokers in the apical periodontitis events (Figure 2). Likewise, for teeth, we included 3 studies [222326] and found an OR of 1.71, 95% CI (0.99–2.93), and I2 = 72%. We did not find any differences (Figure 3). Nonetheless, there was high heterogeneity in the 2 analyses, making it difficult to interpret these results.
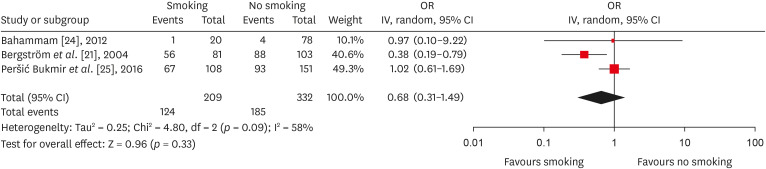
Forest plot of association between root canal treatment with apical periodontitis in smokers vs non-smokers subjects (analysis by patients).
OR, odds ratio; CI, Confidence interval.
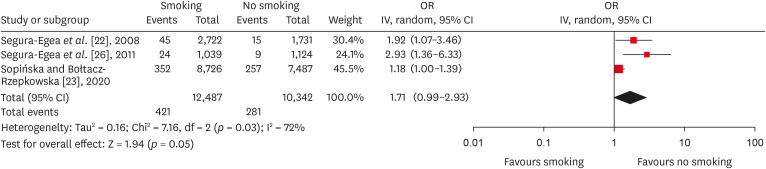
Forest plot of association between root canal treatment with apical periodontitis in smokers vs non-smokers subjects (analysis by teeth).
OR, odds ratio; CI, Confidence interval.
Sensitivity analysis
There were no changes in the estimated effect when performing the sensitivity analysis.
DISCUSSION
Evaluation of the 6 articles included in this systematic review suggests that apparently and under the limitations of this study, there were no statistical differences in the prevalence of post endodontic AP when comparing non-smokers vs smoker subjects regarding patients (OR, 0.68; 95% CI, 0.31–1.49; I2 = 58%) and teeth (OR, 1.71; 95% CI, 0.99–2.93; I2 = 72%).
The apical osteolytic lesion is the result of the dynamic encounter between bacteria and the immune system in an attempt of the host to prevent endodontic bacteria from spreading into the alveolar bone or even to distant organs. Bacteria emerging from the infected root canal provide a continuous stimulus for the recruitment of polymorphonuclear granulocyte neutrophils at the periapical level in order to contain and phagocytize such bacteria [27].
Chronic exposure to endodontic pathogenic bacteria or their sub-products may result in the local production by plasma cells of specific IgG to endodontic bacteria, which in turn will activate the complement system, thus amplifying the immune reaction [2829]. However, this dynamic encounter between bacteria and the immune system also causes local bone damage in the form of an osteolytic lesion. During the apical inflammatory reaction, different cytokines such as IL-1β and TNF-β (which are the primary causes of the local bone lysis) are generated, which in turn, initiate and maintain an osteoclastic response through the activation of the receptor activator of nuclear factor kappa-B ligand (RANKL)–RANK molecular complex [27303132]. When a successful RCT eliminates the pathogenic endodontic bacteria, the inflammatory apical reaction together with the osteoclastic activity will cease to exist and the local osteogenic potential will take over, as it has been demonstrated that osteoprogenitor cells are present within the apical lesion [303334]. Osteogenic cells provide the apposition of a new bone matrix, followed by cycles of bone remodeling which will finally end up in the periapical healing of the bone defect [3132]. Ørstavik [35] found that complete healing of AP may require up to 4 years, however, signs of periapical healing were visible in at least 89% of the cases after 1-year of follow-up. Ng et al. [36] in a random-effects meta-analysis, revealed that the weighted pooled healing success rate of AP was 29.6% over a 6-month time period. Siqueira et al. [37] found that AP shows clear repair criteria compatible with successful RCT in 75% of cases in a 2-year follow-up period. Azim et al. [38] reported that the average time required for complete healing of an AP was 11.78 months.
On the other hand, it has been reported that a range of toxic substances such as nicotine, carbon monoxide, and hydrogen cyanide released during combustion and pyrolysis of the tobacco, would probably have a negative impact on the healing of AP [39], since such toxicants may potentially cause endothelial cell injury and affect the microvasculature of the periapical tissues, which in turn, could lead to a lower contribution of nutrients and oxygen, both essential in healing processes [4041]. Furthermore, tobacco smoking has been associated with fibroblast dysfunction, thus leading to impaired tissue repair [4042].
However, the 6 articles included in this review, agreed to suggest that there is no association between the prevalence of post endodontic AP and CS, in contrast to 2 recent systematic reviews that reported a negative influence of smoking on periapical disease in endodontically untreated teeth in terms of the prevalence of AP [1718]. Therefore, it could be hypothesized that once the intraradicular microbial component causing the periapical inflammatory phenomenon has been removed, the molecular healing processes of AP could not be completely altered as a consequence of the local and systemic deleterious effects inherent to the habit of smoking and therefore smoking behavior should not be considered as a risk factor for the failure of endodontic therapy.
This is in line with Marending et al. [43] who reported that smoking is not a factor affecting the outcome of orthograde root canal therapy in the long term and Touré et al. [44] who found that smoking is not a factor related to failure or extraction of Endodontically Treated Teeth. Further, Danin et al. [45] suggested that the concentration of some proinflammatory cytokines such as TNF-α and transforming growth factor-beta 1 (TGF-β1) in AP does not differ in smokers vs non-smokers.
As the most important strength, we carefully followed Cochrane’s recommendations to perform this systematic review and meta-analysis. Moreover, to the best of our knowledge, this is the first systematic review that assessed the prevalence of AP associated with RCT in non-smokers vs smoker patients. On the other hand, this study has several limitations. First, all the studies included in this systematic review were of cross-sectional design [212223242526], which does not assess variables such as: if the post endodontic AP is healing or not, the diagnosis prior to endodontic therapy, who and how was carried out the RCT (a general dentist or an endodontist and the techniques and materials used). Therefore, longitudinal studies would be very useful to evaluate the evolution of the AP in the long term and at the same time avoid the overestimation of AP. Secondly, the identification of AP in the 6 articles included in this systematic review was carried out by using 2- dimensional imaging techniques (Panoramic and or Periapical radiographs), which although accepted for the identification of AP as they provide reliable results under lower radiation doses, have great limitations in estimating the presence and size of AP and possess lower precision and sensibility when compared to cone-beam computed tomography [174647]. Further, although the periapical index (PAI) is currently the gold standard index for the evaluation of AP at the radiographic level, only 3 studies [222526] applied this evaluation method, and the remaining studies [212324] designed their own evaluation criteria, which compromises the possibility of comparison among studies due to lack of standardization. Finally, in 5 of the 6 studies of this systematic review, smoking was analyzed as a dichotomous variable, however, the influence of aspects such as intensity, duration, and amount of smoking habit was not reported [2122242526]. Only one study done by Sopińska and Bołtacz-Rzepkowska [23] categorized the history of smoking (smokers: “subjects who had been smoking in the past for 5 years without interruption, at least 10 cigarettes a day”).
In view of the foregoing, it is important to emphasize that results from this systematic review are inconclusive, as there is a lack of well-designed clinical studies with longitudinal designs that allow to clearly elucidate the influence of CS on the prevalence of post endodontic AP.
CONCLUSIONS
Our findings suggest that there was no association between CS and post endodontic AP, as we did not find statistical differences in the prevalence of post endodontic AP when comparing non-smokers vs smoker subjects. Therefore, CS should not be considered a risk factor associated with endodontic failure. Nonetheless, there were important limitations that prevent the extrapolation of these results. We strongly suggest improving the quality of studies to improve the strength of these results.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: Ríos-Osorio N.
Data curation: Jiménez-Peña O, Muñoz-Alvear HD.
Formal analysis: García-Perdomo HA.
Investigation: Quijano S, Caviedes-Bucheli J.
Methodology: Muñoz-Alvear HD, Jiménez- Peña O, Caviedes-Bucheli J.
Project administration: Ríos-Osorio N.
Software: Muñoz-Alvear HD.
Supervision: Jiménez-Castellanos FA.
Validation: Quijano S, Caviedes-Bucheli J.
Visualization: Quijano S.
Writing - original draft: Ríos-Osorio N.
Writing - review & editing: Ríos-Osorio N, Jiménez-Castellanos FA, García-Perdomo HA.
Appendices
Appendix 1
Search strategy translated for each database