Deep proximal margin rebuilding with direct esthetic restorations: a systematic review of marginal adaptation and bond strength
Article information

Abstract
This review aimed to characterize the effect of direct restorative material types and adhesive protocols on marginal adaptation and the bond strength of the interface between the material and the proximal dentin/cementum. An electronic search of 3 databases (the National Library of Medicine [MEDLINE/PubMed], Scopus, and ScienceDirect) was conducted. Studies were included if they evaluated marginal adaptation or bond strength tests for proximal restorations under the cementoenamel junction. Only 16 studies met the inclusion criteria and were included in this review. These studies presented a high degree of heterogeneity in terms of the materials used and the methodologies and evaluation criteria of each test; therefore, only a descriptive analysis could be conducted. The included studies were individually evaluated for the risk of bias following predetermined criteria. To summarize the results of the included studies, the type of restorative material affected the test results, whereas the use of different adhesive protocols had an insignificant effect on the results. It could be concluded that various categories of resin-based composites could be a suitable choice for clinicians to elevate proximal dentin/cementum margins, rather than the open sandwich technique with resin-modified glass ionomers. Despite challenges in bonding to proximal dentin/cementum margins, different adhesive protocols provided comparable outcomes.
INTRODUCTION
Aesthetic restorations are in high demand in the posterior region, especially because restorations can be made with adhesive resin restorative materials, which protect the intact tooth structure without sacrificing sound tooth structure for mechanical retention [1]. Current adhesive technology and modern resin composite materials contribute to the restoration of severely damaged teeth using directly placed resin composite restorations [2].
Although subgingival cavities with cervical margins extending below the cementoenamel junction (CEJ) represent a very common clinical situation, they generate significant technical and operative challenges in restorative dentistry, including partial or total loss of sealing of cervical margins in the absence of enamel [3]. Bonding to the etched enamel has proven to be efficient, stable, and durable [4]. However, adhesion to dentin is more challenging due to its high organic component, tubular structure, and permeability, along with its lower surface energy [5]. In addition, the margins located below the CEJ are cementum-limited. The presence and thickness of this outer layer of cementum may explain the difficulty in achieving adhesion in these areas [6].
To facilitate the direct or indirect restoration of proximal cavities with dentin/cementum cervical margins, 2 techniques have been proposed. The first is the “sandwich technique,” in which a glass ionomer cement (GIC) is applied at the gingival margin of the cavity until below the proximal contact, and then covered with a direct resin composite [7]. This technique has advantages including fluoride release, moisture tolerance, and intrinsic adhesion to the glass ionomer (GI) with dental tissues [8]. However, high clinical failure rates have been reported when GIC was used with this technique [9]. Therefore, modifications using resin-modified glass ionomers (RMGIs) and high-viscous GIs have been developed, with acceptable long-term results [1011]. The second technique, described by Dietschi and Spreafico, involves the gradual relocation of the deep proximal margins, which is performed using a resin-composite base to uplift the cavity outlines to facilitate the next steps for indirect restorations. This is called proximal box elevation (PBE) [12].
Several researchers have advocated for the use of resin composites for bonding to proximal dentin/cementum margins, especially with the current types of adhesives [913]. However, some recent studies have argued that GIs, with their hydrophilic nature, flexibility, and chemical bonding, could be a more suitable option for bonding to deep, moist dentin/cementum margins [1415]. Consequently, debate continues regarding the best restorative material and adhesive protocol to use with such margins, especially with the current huge commercial variety of restorative materials and adhesive systems. Therefore, the aim of this systematic review was to find an answer to this argument based on the scientific available data.
MATERIALS AND METHODS
The PICO framework
With reference to the problem (P), intervention (I), comparator (C), and outcome (O) (PICO) framework [16], the research questions of this systematic review were:
1. What is the potential best direct restorative material (C) in terms of marginal adaptation and bond strength (O) to elevate (I) the dentin/cementum cervical margins in class II cavities to be restored with direct restoration (P)?
2. What is likely to be the most suitable adhesive protocol (C), in terms of marginal adaptation and bond strength (O), that should be used with restorative materials to bond to (I) dentin/cementum cervical margins in class II cavities to be restored with direct restoration (P)?
Information source and systematic search
The review methodology was based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [1617].
Three electronic databases were investigated in this systematic review: the National Library of Medicine (MEDLINE/PubMed), Scopus, and ScienceDirect. The following keywords and Medical Subject Headings (MeSH) were used to search these database: “subgingival cervical margin,” “cervical marginal adaptation,” “proximal marginal adaptation,” “cervical marginal quality,” “proximal marginal quality,” “bonding to gingival dentin,” “bond strength to proximal deep margin,” “proximal deep margin,” “deep margin elevation,” “proximal direct restoration,” “open sandwich technique,” and “bilayered resin composite.” Resources that were not available on the internet were manually checked. Then, the identified articles were imported into Endnote X7.7 software (Thompson Reuters, Philadelphia, PA, USA) to remove duplicates. A gray literature search was conducted following the online database search.
Search strategy
After removal of the duplicates, all articles identified through the searches were compiled, printed, and distributed to all authors. Eligibility criteria for all studies were checked individually by each author. The articles were selected based on 1) the relevance of the title, 2) the relevance of the abstract, and 3) the analysis of the full text. The included studies were laboratory studies that investigated the effect of restorative materials and/or adhesive protocol types on marginal adaptation and the bond strength of the cervical interface between the material and dentin or cementum in class II cavities to be restored with direct restoration. At least 3 authors had to agree for a study to be included in the current review.
Assessment of risk of bias
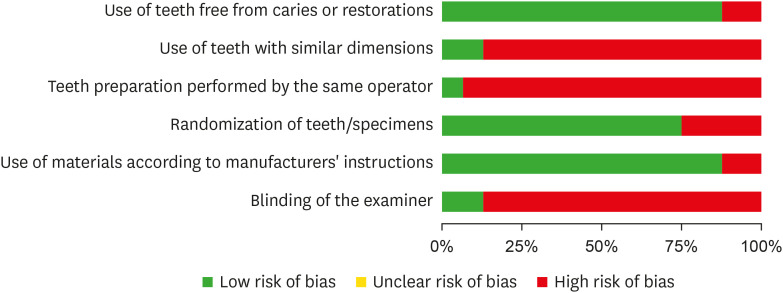
The risk of bias was independently assessed by 3 authors based on the parameters used in previous systematic reviews of laboratory studies [1819]. The evaluated parameters were: use of teeth free from caries or restorations, use of teeth with similar dimensions, teeth preparation performed by the same operator, randomization of teeth/specimens, use of materials according to manufacturers’ instructions and blinding of the examiner. If a parameter was reported to be used in the study, “yes” was assigned for that parameter. If the information was missing, or if the parameter was not reported, then “no” was assigned for that parameter. Articles that reported 1 or 2 parameters were classified as having a high risk of bias. Those reporting 3 or 4 parameters were considered as having a medium risk of bias, whereas those reporting 5 or 6 parameters were classified as having a low risk of bias. The risk of bias graph and summary for the selected studies were obtained by RevMan 5.3.
RESULTS
Search results
Electronic searches yielded 2,244 published articles. After the removal of duplicates and articles not in English or published before 2010, the titles/abstracts of 566 search results were independently evaluated by the authors. However, 474 studies were excluded for 1 (or more) of the following reasons: not being in the dental field; being published in conference proceedings or a book section; having a study design of case report, clinical trial, or review article; dealing with implant-supported restorations or endodontically treated teeth; not using human permanent teeth; and not being related to the research question.
Ninety-two studies were assessed in full-text form for eligibility. Following the inclusion and exclusion criteria, 76 studies were excluded. The excluded studies evaluated marginal adaptation or bond strength for margins below the CEJ in class V cavities, restored with indirect restorations, or placed above or in the CEJ. Finally, 16 studies fulfilled the originally set inclusion criteria for this review. The research stages are illustrated in the flowchart (Figure 1).
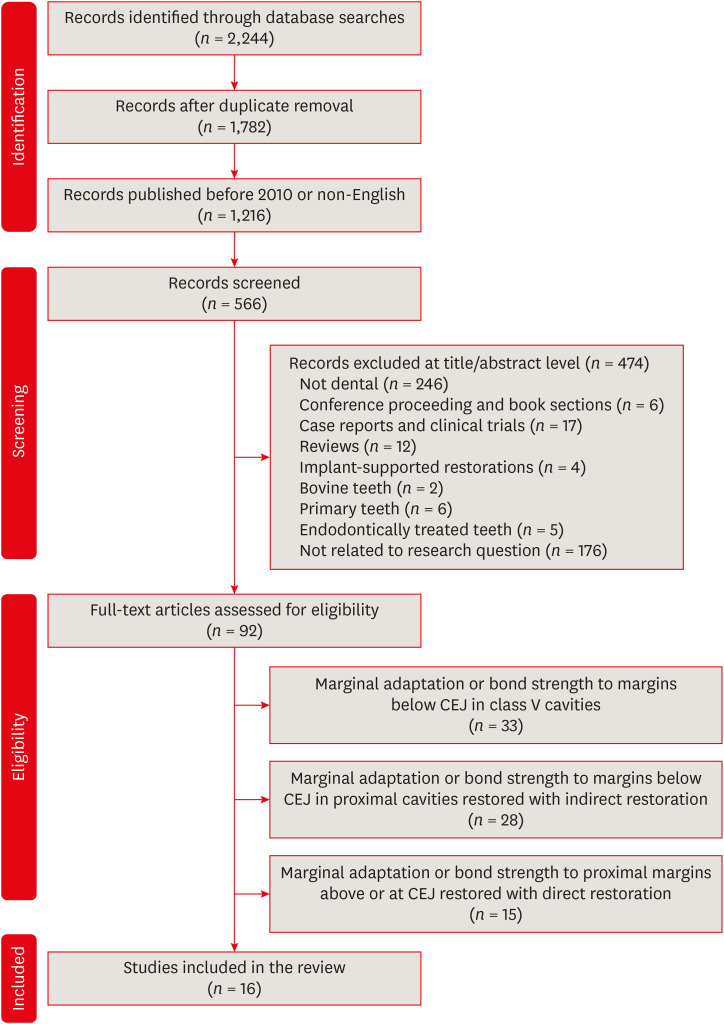
Search flowchart as adapted from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.
CEJ, cementoenamel junction.
Data extraction
Since the selected studies had a high degree of heterogeneity in terms of different materials, methodologies, and evaluation criteria within each test, a meta-analysis was not appropriate for any of the included tests (Tables 1 and 2).

Assessment of sample sizes, test types, and aging methodologies

Scientific categories, brand names of restorative materials, and adhesives used
Descriptive analysis
The current review evaluated 16 studies [20212223242526272829303132333435]. Twelve studies (75%) evaluated marginal adaptation, while 5 studies (30%) evaluated micro-tensile bond strength (μTBS) between the restorative materials and proximal dentin/cementum margins [20212223242526272829303132333435].
Twelve studies (75%) used a type of aging, including thermal cycling, mechanical loading, thermo-mechanical loading, storage in phosphate-buffered saline, and storage in water [202123242527282930323334]. A summary of different aging methodologies utilized is presented in Table 1. Eleven studies used human molars while 4 studies used human premolars [202122232425272829303132333435]. One study used both types of teeth [26]. Different restorative material categories and viscosities were used in the included studies. Scientific categories and brand names of all materials used in addition to their adhesive protocol within the studies are illustrated in Table 2.
After a careful assessment of the included studies, the primary 5 parameters discussed in the results for each test were: 1) the open sandwich technique (OST) with GIs, 2) OST with flowable composites, 3) flowable bulk-fill composites, 4) Silorane-based composites, and 5) effect of the bonding protocol.
1. Assessment of marginal adaptation
1) Testing methodology
(1) Finishing and polishing of gingival margins pre-test
All finishing and polishing (F/P) studies were performed for restored gingival margins except for 1 study that depended only on matrix adaptation for preventing any overhanging restoration [34]. One study made an additional step besides F/P, cleaning the resin-dentin interface with 37% phosphoric acid for 5 seconds [20]. All the studies performed immediate F/P after restoration, except for 2 studies that delayed this step by 1 week [2632].
(2) Direct or replica
Four studies examined the adaptation of restorations directly on the specimens while 8 studies used epoxy resin replicas, three of which examined 2 sets of replicas before and after aging [202123242627282931323334].
(3) Examination method
All studies assessed marginal adaptation by scanning electron microscopy (SEM) except for 1 study that used metallographic light microscopy [26]. Furthermore, 1 study used the FDI ranking of marginal quality using loupes and explorers to compare their results with SEM results for the same specimens [21]. The different magnifications used in each study are illustrated in Table 3.

Assessment of marginal adaptation evaluation methodologies
(4) Number of margins assessed
Three studies prepared 2 cavities in the same tooth, above and below the CEJ, and then evaluated adaptation in both enamel margins on one side and dentin gingival margins on the other side [212332]. Three studies evaluated tooth restoration interface of both proximal enamel and proximal and cervical dentin of the same restored cavity [293133]. All studies evaluated external marginal adaptation, except for 1 study that evaluated internal adaptation as well [26]. The exact margins that were evaluated in each study are shown in Table 3.
(5) Criteria for evaluation
Marginal adaptation was calculated as the percentage of the continuous margin to the total margin length in 8 studies [2021242728293133]. However, the scoring differed among these studies for either the continuous (perfect) margin or gap. Three of them scored the margin as perfect if the interface was continuous or had a gap of less than 1 µm in length [202428]. Five other studies [2127293133] scored the margin as perfect if it had no gaps with any length and was completely uninterrupted, and one used the FDI ranking of marginal quality [21]. One study measured adaptation by categorizing the bonding sites as adequate or inadequate; the inadequate category accounted for the detachment of restorative materials from the tooth or the presence of cracks in either restoration or the tooth structure itself [26]. One study measured the widest interfacial gap in each specimen in microns [23]; furthermore, 2 studies observed the quality of the margins qualitatively without scoring, measuring, or using any statistical tests [3234]. The summary of marginal adaptation evaluation methodologies is shown in Table 3.
2) Assessment of marginal adaptation results
(1) OST with RMGI
One study used the OST with nanofilled RMGI under a nanohybrid composite with all bonding strategies and found a significant increase in the quality of margins compared to using the resin composite without liner [28]. When the same category was used with the same technique under both nanofilled and nanohybrid composites and was compared with calcium silicate materials (CSMs) (e.g., mineral trioxide aggregate [MTA] or Biodentine), the percentage of perfect margins was higher in the nanofilled RMGI and Biodentine groups than in the MTA group [24]. In contrast, 1 study qualitatively analyzed the marginal adaptation of RMGI using the OST under a microhybrid composite and observed wider gaps between the material and dentin/cementum margin than when using resin composite alone or dental amalgam [32]. One study compared 3 GI-based liners under a microhybrid composite in the OST in terms of internal and external marginal adaptation, revealing that RMGI had the highest percentage of adequate margins, followed by nanofilled RMGI and GIC [26].
(2) OST with flowable resin composites
The utilization of flowable composite in OST did not significantly differ in the percentages of continuous margin relative to using a heavy body and microhybrid or nanofilled composites without a flowable liner with both etch-and-rinse (ER) and self-etch (SE) adhesives [212331]. This finding was valid for another study that compared the OST using a 1-mm flowable composite with a nanohybrid composite without a flowable liner [29]. In contrast, 1 study found that the percentages of continuous margin were significantly higher in the OST with flowable composites than with nanohybrid composites [28]. In addition, 1 study made a qualitative assessment for gingival margins restored with flowable liner and microhybrid composites, and this study revealed more adequate and smooth margins without voids or gaps in the flowable composite group [34].
(3) Effect of different liner thicknesses
One study compared different thicknesses (1 mm, 4 mm) of the flowable microhybrid composite placed in OST and reported a significant reduction in the percentage of continuous margins in the 4-mm thickness flowable composite group than the group with 1-mm thickness [29].
(4) Flowable bulk-fill composites
The use of flowable bulk-fill composites did not provide additional benefits in terms of marginal adaptation at the dentin/cementum margins using SE adhesives compared to microhybrid, nanofilled, or silorane composites [31]. This was true for other 2 studies that compared nanohybrid composites with ER adhesives [2729]. Similar findings were found in 2 other studies comparing this category with heavy-body microhybrid, regular bulk-fill, and sonic fill composites with both ER and SE adhesives [2123].
(5) Silorane-based composites
One study demonstrated that the best marginal adaptation of a silorane-based composite was obtained when bonded to an SE adhesive, followed by a silorane-specific adhesive. In addition, they found that this bonding protocol enabled the material to perform better, not only compared to using its specific adhesive, but also compared to microhybrid and nanofilled resin composites bonded with SE adhesives [31].
(6) The effect of different bonding protocols
The bonding protocol and the type of adhesive were not significant in marginal adaptation values in the OST with a flowable composite bonded using ER and SE adhesives, or even with different ER adhesives (acetone-based vs. ethanol-based) [202128]. Similar findings were found when the OST was performed with nanofilled RMGI and CSMs, which were then bonded to the overlying resin composite with ER and SE adhesives [2428]. This was true for nanohybrid, heavy-body microhybrid, and regular and flowable bulk-fill composites, as well as sonic-fill composites bonded using different adhesives [2128].
2. Assessment of μTBS between restorative materials and tooth structure
1) Testing methodology
(1) Testing machine and crosshead speed
Three studies tested specimens with a universal testing machine, while 1 study used a microtensile tester [22233035]. Two studies used a crosshead speed of 1 mm/min [2230], and 2 other studies used a crosshead speed of 0.5 mm/min [2335]. One study did not specify the crosshead speed of the testing device [25].
(2) Shape and number of bonded specimens (beams)
Three studies accounted for hourglass-shaped specimens while 2 studies used rectangular sticks [2223253035]. Two studies obtained 3 specimens per restoration, and 2 other studies obtained only 2 specimens [222330]. Moreover, 1 study did not specify the number of beams from each tooth [25].
(3) Cross-sectional surface area of the bonded specimen
Four studies used a surface area of 1 mm2 for the bonded interface [22253035]. On the contrary, 1 study did not report the exact surface area [23].
(4) Type of margins and walls examined
Three studies evaluated the μTBS of materials bonded to only the dentin/cementum margin, while 1 study evaluated it at both enamel and dentin/cementum margins (2 box cavities in the same tooth, above and below the CEJ) [22232530]. One study evaluated the μTBS at different preparation walls of the same specimen (pulpal, axial, and gingival walls) [35].
(5) Method of failure analysis
Failure modes were recorded using stereomicroscopy (40×) in 2 studies and light microscopy (50×) in 1 study, whereas 1 study did not report the method [22232535]. One study performed an additional SEM analysis (500×) on 2 of the failed specimens from each group [23].
(6) Scoring of failure types
One study recorded the modes of failure as follows: 1) cohesive failure in dentin, 2) adhesive failure between the hybrid layer and dentin, or 3) cohesive failure in the restoration [22]. Two other studies used the same scores in addition to a fourth one: 4) mixed failure (adhesive + cohesive in either resin or dentin) [2325]. Moreover, 1 study recorded the number of specimens that had premature failure in each group, and this failure occurred mainly during specimen preparation at the point of hourglass shaping [35]. In addition, 1 study did not assess the failure mode [30]. Two studies recorded the failure mode as the percentage of each type of failure in each group while the third study recorded the number of cases of each mode [222325].
(7) Calculation of μTBS values
In all studies, the bond strength was expressed in megapascals, dividing the load at failure in newtons by the bonding surface area in millimeters squared. One study mentioned that 1 beam out of 2 per restoration was randomly chosen for the test while another study obtained the μTBS value by obtaining the arithmetic mean of μTBS values for the different beams per restoration [2335]. A summary of μTBS test methodologies is presented in Table 4.

Assessment of microtensile bond strength testing methodologies
2) Assessment of μTBS results
(1) OST with RMGI or flowable composites
Two studies investigated μTBS of microhybrid and nanofilled resin composite with different adhesives without any lining compared to the OST with flowable composites and with RMGIs [2330]. They found that the RMGI group had significantly lower bond strength values with the proximal dentin/cementum margins, followed by the flowable composite group, especially after aging [30].
(2) Flowable bulk-fill composites
Two studies found that the μTBS of flowable bulk-fill composites was higher than that of nanofilled, regular bulk-fill, and microhybrid heavy-body composites when used with ER adhesives, even when changing the filling technique (bulk fill technique or incremental technique) [2223]. In contrast, 1 study found that a microhybrid composite had higher bond strength than a flowable bulk-fill composite when bonded using the SE protocol [25].
(3) Silorane
One study reported higher bond strength of a silorane-based composite with an ER adhesive than either regular bulk-fill or microhybrid heavy-body resin composites with the same adhesive [23].
(4) The effect of different adhesive protocols
Two studies found that bonding of different restorative materials with ER adhesives resulted in higher bond strength values than using SE adhesives [2335]. On the contrary, 1 study found significantly higher bond strength when using an SE adhesive with microhybrid composite than when using an ER adhesive [25].
Risk of bias assessment
According to the parameters considered in the analysis, 11 studies (69%) presented a medium risk of bias [2021222324262729323335], and 5 studies (31%) presented a high risk of bias [2528303134]. The risk of bias graph and summary are illustrated in Figures 2 and 3.
Risk of bias summary.
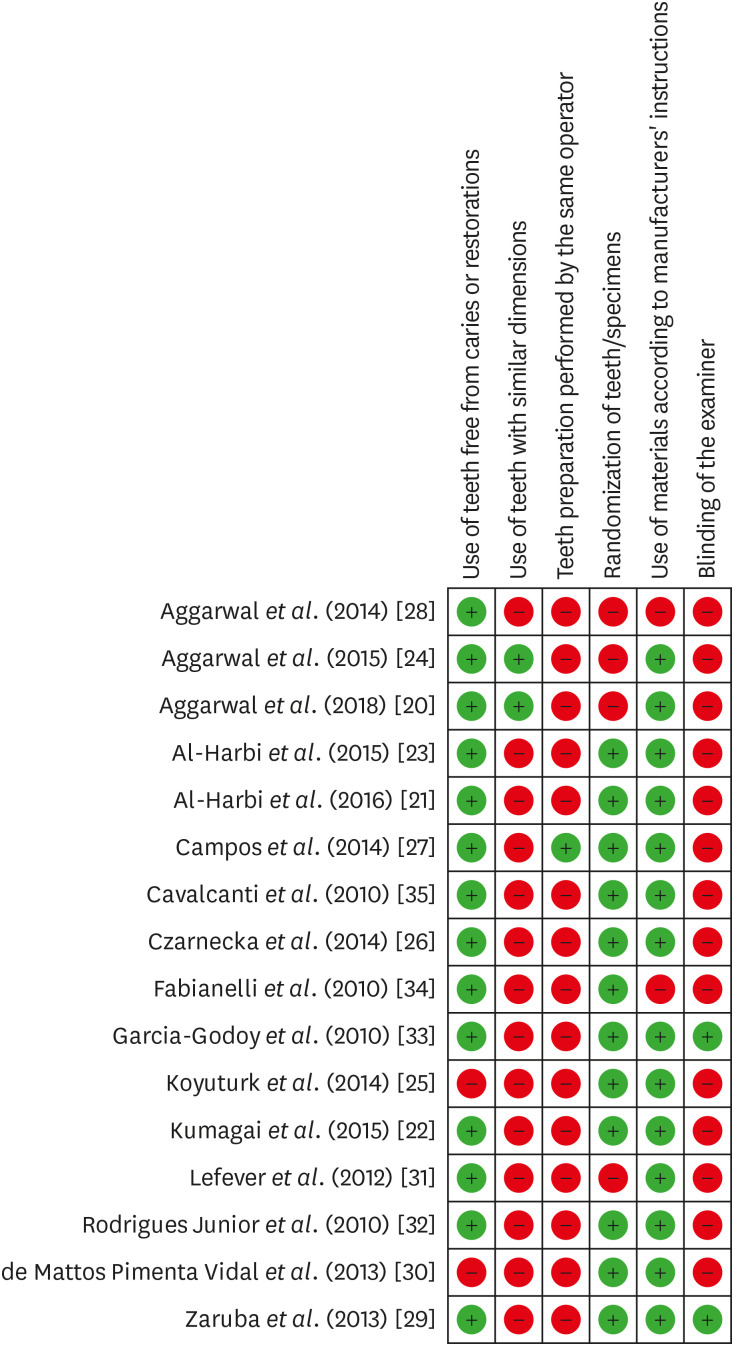
Risk of bias summary.
DISCUSSION
Rationale
The rapid development of dental adhesives and restorative materials led the authors of this review to limit the inclusion of studies from the last 10 years, while excluding previous scientific knowledge from investigations of older generations of restorative materials and adhesives that may not be commercially available anymore.
Two very recent clinical studies involving periodontal evaluation of PBE under direct and indirect restorations found normal gingival healing during follow-up [3637]. This papillary healing may jeopardize the clinical examination of the subgingival tooth/restoration margins. This is why no clinical studies in the 10-year period of this review were performed to evaluate in vivo marginal quality for subgingival dentin/cementum proximal margins. Furthermore, no randomized clinical trial or retrospective or prospective clinical study evaluating the periodontal response with the use of different base materials for proximal margin elevation were found during the same search period; therefore, this review included only laboratory studies.
The rationale for including these laboratory tests in this review was based on the widely-acknowledged principle in restorative dentistry that in order to increase the survival probability of the restoration, the transition between the restorative material and the tooth structure must be continuous [38]. The evaluation of an in vitro marginal seal can be performed by measurement of marginal adaptation to observe the same marginal aspect after storing or stressing the same specimens [21]. Bond strength tests were also included, as they assess the ability of a restorative material or dentin bonding system to establish a bond between the restorative material and the biological substrate (dentin and/or enamel), which might affect the uniform seal between both substrates [23].
OST with GIs
The intrinsic adhesion of GIs to dentin was reported to secure the sealing in deep root-reaching cervical deep cavities, especially in patients with a high risk of caries [2439]. This is also less technique-sensitive than resin composites concerning moisture control in such cavities [40]. Regardless of these data, this review found that the OST with RMGIs showed wider gaps with dentin margins and less μTBS than resin composite without liner [3032]. This could be related to the high viscosity of RMGI used in the studies, which created less homogeneous and more brittle restorations than using resin composite with a proper layering technique. Some researchers have stated that RMGIs in the OST detach from the dentin/cementum mainly in the initial stages of maturation due to polymerization stresses of the overlying resin composite [41].
On the contrary, another study reported better marginal quality in RMGI and GIC OST groups [28]. This discordant result could be related to the fact that this study conditioned the gingival margins in this study with an RMGI-specific primer before GI application, which is an important step for proper hybridization of any type of GI. This was not performed in earlier studies, and this conditioning can favorably affect the quality of bonding, counteracting the pulling effect of shrinkage of the overlying composite.
OST with flowable composites
Although some authors have recommended using flowable composite liners with a low elastic modulus under resin composite, they may act as stress-absorbing layers that cause a reduction in polymerization shrinkage of the overlying composite with better marginal adaptation [2834]. Others have found no benefit in using them to enhance marginal integrity or bond strength [23293031]. Flowable composites have reduced filler content that may be associated with high polymerization shrinkage. Consequently, a thinner flowable increment is associated with a lower shrinkage percentage and better conversion rate, as was reported by de Goes et al. [42]. This can explain the deteriorating marginal adaptation reported by recent studies, which used 2-mm-thick gingival increments for the flowable composite compared to the 0.5- to 1-mm-thick increments used in the former studies [21242834].
The low viscosity and reduced filler content of flowable resins may result in reduced creep strain, which leads to a high amount of shrinkage and less stiffness than regular resin composites resulting in stress similar to that obtained with nonflowable materials [43]. This finding could explain the lower bond strength of the flowable layer compared to regular resin composite, especially after simulation aging [2330].
Flowable bulk-fill composites
No further benefits were found from using a flowable bulk-fill composite that was placed in the cavity in 4-mm bulk compared with other layered composites in terms of marginal adaptation, even when using different adhesives [212325272931]. In addition, the thickness of the flowable bulk-fill composite—either 1 or 4 mm—did not make any difference [29]. Nevertheless, the ability of this material to be applied and light-cured in bulk could be considered an advantage [21]. Proximal dentin/cementum margins are usually accompanied by deep and large cavities, which would benefit from quick application and reduced restorative procedure time and effort, in addition to minimized air void entrapment and improved quality of the final restoration [9212244]. The similar sealing quality of layered composites and different thicknesses of bulk-fill composites was explained by previous reports [4546]. They attributed this to the low volumetric shrinkage in addition to the low elastic modulus of flowable bulk-fill composites, which was hypothesized to be more important than shrinkage for determining the stresses. That led to reduced polymerization contraction stresses, which in turn compensated for bulk curing of these composites.
It was found that the bond strength of flowable bulk-fill composites was higher than that of incremental composites when used with ER adhesives, even with changing the filling technique [2223]. This could be due to the type of flowable bulk-fill composite used in the included studies. It was more translucent than incremental composites, which led to more light penetration, and consequently resulted in a higher degree of conversion and ideal polymerization to the full thickness with the standard light energy that favorably affected bond strength [47]. Contrary to the previous results, 1 study found that incremental microhybrid composites had greater bond strength than a flowable bulk-fill composite when used with SE adhesive [25]. This conflicting outcome may be explained by the different bonding protocols used.
The results regarding failure patterns in the studies were variable, but the adhesive/mixed failure patterns were still the predominant failure modes [222325]. This could be due to differences in classification types of failure mode among the studies, and also differences in crosshead speed, which was reported to affect the failure pattern in a previous systematic review [48].
Silorane-based composites
Silorane-based composites with their specific adhesive provided better marginal quality and higher bond strength than methacrylate-based composites regardless of the bonding approach [2331]. This is in accordance with previous studies, which found that the reduced polymerization shrinkage of silorane led to low contraction stress at the bonding interface, and also superior resistance to thermo-load cycling compared to that of methacrylate-based composites [49].
Bonding protocol
There was no clear effect of different bonding protocols or types of adhesives on marginal adaptation [20212428]. However, 1 study reported a significant reduction in the values of continuous margins when a 1-step SE adhesive was used compared to ER and 2-step SE adhesives. This could be because the 1-step SE adhesive has methacrylated phosphoric esters and 2-hydroxyethyl methacrylate (HEMA) as functional monomers that are hydrophilic in nature; consequently, this adhesive may act as a semi-permeable membrane leading to water imbibition and degradation of resin–dentin bonds [50].
The effect of different adhesive protocols on bond strength between restorative materials and gingival dentin was variable. Two studies stated that tested restorations exhibited better bond strength values when tested with ER adhesives compared to the SE approach [2335]. The better performance of the ER bonding protocol could be explained by the deep demineralization created by phosphoric acid, in addition to the short distance between the adjacent dentinal tubules enabled the adhesive monomers to penetrate, not only from the exposed dentin surface, but also from the lumens of the dentinal tubules to the surrounding demineralized dentin [51]. However, 1 study reported results inconsistent with the previous studies, as they found significantly better bond strength for the SE adhesive compared to the ER adhesive [25]. There could be 2 reasons for this. The former studies trimmed the microrod into an hourglass shape to concentrate the stress at the sites of bonding and to correlate failures to the bonding interfaces, rather than the rectangular bonded sticks tested in the latter study [232535]. The other reason is that the latter study used an acetone-based ER adhesive compared to ethanol-based adhesives in the former studies. In previous laboratory and clinical studies, the ethanol-based bonding systems resulted in higher μTBS and a better retention rate than the acetone-based systems [5253].
Limitations and recommendations
This review is subject to some limitations, such as the exclusion of non-English manuscripts and variations in test materials and techniques, aging methodologies, types of teeth, and the sizes of cavities. This may have led to variations in the results and prevented quantitative analyses of data, including a meta-analysis.
The authors recommend that the laboratory methods for each test should comply with internationally accepted standards in order to be standardized and validated and to allow comparison of material data across studies. Some recent restorative materials and adhesives were not studied sufficiently or even at all, such as glass hybrids, bioactive composites, and antibacterial adhesives despite their promising results in the literature [395455]. Finally, clinical studies concerning non-invasive evaluations of marginal quality for subgingival dentin/cementum margins elevated by different restorative materials and adhesives are needed.
CONCLUSIONS
In light of the currently available scientific evidence, the following conclusions can be drawn: Considering the reduced time and effort in placement of bulk-fill composites (regular or flowable, in addition to sonic fill), they may be recommended to restore proximal cavities with dentin/cementum gingival margins—followed by silorane-based composites, with their specific adhesive, and regular methacrylate-based composites, respectively. In contrast, the OST with RMGIs should be limited to situations in which moisture control is difficult or there are deep cervical cavities in patients at high risk of caries. Despite the challenges encountered during bonding to proximal dentin/cementum margins, different adhesive protocols have provided comparable outcomes.
Notes
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of interest: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Author Contributions:
Conceptualization: Ismail HS, Ali AI, Mahmoud SH.
Data curation: Ismail HS.
Formal analysis: Ismail HS, Mehesen RE.
Investigation: Ismail HS.
Methodology: Ali AI, Mehesen RE.
Supervision: Mehesen RE, Juloski J, Garcia-Godoy F, Mahmoud SH.
Visualization: Mehesen RE.
Writing - original draft: Ismail HS.
Writing - review & editing: Ali AI, Mehesen RE, Juloski J, Mahmoud SH.



